National Institutes of Health (NIH)
National Institute on Drug Abuse (NIDA)
All applications to this funding opportunity announcement should fall within the mission of the Institutes/Centers. The following NIH Offices may co-fund applications assigned to those Institutes/Centers.
Division of Program Coordination, Planning and Strategic Initiatives, Office of Disease Prevention (ODP)
UM1 Research Project with Complex Structure Cooperative Agreement
- August 31, 2022- Implementation Changes for Genomic Data Sharing Plans Included with Applications Due on or after January 25, 2023. See Notice NOT-OD-22-198.
- August 5, 2022- Implementation Details for the NIH Data Management and Sharing Policy. See Notice NOT-OD-22-189.
RFA-DA-25-061 , U24 Resource-Related Research Project (Cooperative Agreements)
RFA-DA-25-062 , R01 Research Project
See Section III. 3. Additional Information on Eligibility.
The intersection of the criminal-legal system and the community-based healthcare system is a critical target for addressing the overdose crisis. Given the recent evolution of both the epidemiology of the overdose crisis and public policies intended to support overdose prevention efforts, new research is needed to take effective interventions to scale in law enforcement, jails, courts, and community corrections. There is also a pressing need to rigorously test new and emerging models for effectively addressing the complex needs of individuals with substance use disorder (SUD) and/or high overdose risk in these settings. Of particular importance is the coordination of services between public health and public safety agencies, to ensure continuity of care for individuals as they transition between these systems.
To support research on effective interventions and implementation strategies for addressing SUD, overdose risk, and common co-occurring conditions in these populations and systems, the National Institute on Drug Abuse (NIDA) intends to continue the Justice Community Overdose Innovation Network (JCOIN) – Phase II. The purpose of the network is to bring together a national consortium of investigators and practitioner partners to conduct an array of research and capacity building activities to improve the delivery of effective interventions for adults and youth, spanning the key points of the sequential intercept model (i.e., crisis intervention, emergency response, law enforcement diversion/deflection, pre-trial services, courts, jail, prison, re-entry services, probation, parole).
The structure of the network will include multiple research centers, working in collaboration with four complementary resource and support centers. This notice of funding opportunity (NOFO) seeks applications for JCOIN Phase II Clinical Research Hubs.
This Notice of Funding Opportunity (NOFO) requires a Plan for Enhancing Diverse Perspectives (PEDP).
December 22, 2024
| Application Due Dates | Review and Award Cycles | ||||
|---|---|---|---|---|---|
| New | Renewal / Resubmission / Revision (as allowed) | AIDS - New/Renewal/Resubmission/Revision, as allowed | Scientific Merit Review | Advisory Council Review | Earliest Start Date |
| January 22, 2025 | Not Applicable | Not Applicable | June 2025 | August 2025 | September 2025 |
All applications are due by 5:00 PM local time of applicant organization.
Applicants are encouraged to apply early to allow adequate time to make any corrections to errors found in the application during the submission process by the due date.
No late applications will be accepted for this Notice of Funding Opportunity (NOFO).
Not Applicable
It is critical that applicants follow the instructions in the Research (R) Instructions in the How to Apply - Application Guide, except where instructed to do otherwise (in this NOFO or in a Notice from NIH Guide for Grants and Contracts).
Conformance to all requirements (both in the How to Apply - Application Guide and the NOFO) is required and strictly enforced. Applicants must read and follow all application instructions in the How to Apply - Application Guide as well as any program-specific instructions noted in Section IV. When the program-specific instructions deviate from those in the How to Apply - Application Guide, follow the program-specific instructions.
Applications that do not comply with these instructions may be delayed or not accepted for review.
Background
The NIH Helping to End Addiction Long-Term® (HEAL) Initiative: This study is part of the NIH’s HEAL initiative to speed scientific solutions to the national opioid public health crisis. The NIH HEAL Initiative® bolsters research across NIH to (1) improve treatment for opioid misuse and addiction, and (2) enhance pain management. More information about the HEAL Initiative is available at https://heal.nih.gov.
The Justice Community Overdose Innovation Network (JCOIN): The JCOIN has two broad, complementary goals: to build the evidence base for the delivery of substance use disorder (SUD) treatment services for individuals involved in the criminal-legal system, and to build capacity to implement effective services for SUD, overdose prevention, and related co-occurring conditions. Phase I of JCOIN supported a consortium of practitioner-partnered research projects focused primarily on testing strategies to connect individuals with effective opioid use disorder (OUD) treatment at key transition points between the criminal-legal system and community-based healthcare. Phase I supported 13 multi-site clinical trials and more than 50 additional research protocols including surveys, modeling, dissemination, pilot studies and other projects. The network was supported by a Coordination and Translation Center (CTC) and a Methodology and Advanced Analytics Resource Center (MAARC).
Given the recent evolution of both the epidemiology of the overdose crisis and public policies intended to support overdose prevention efforts, new research is needed to take effective interventions to scale in jails, courts, and community corrections, and to rigorously test new and emerging models for effectively addressing the complex needs of individuals with SUD and/or high overdose risk. Of particular importance is the coordination of services between public health and public safety agencies, to ensure continuity of care for individuals as they transition between these systems.
To support research on effective interventions and implementation strategies for addressing SUD, overdose risk, and common co-occurring conditions in these populations and systems, the National Institute on Drug Abuse (NIDA) seeks applications for JCOIN Phase II. The purpose of Phase II is to bring together a national network of investigators and practitioner partners to conduct an array of research and capacity building activities to improve the delivery of effective interventions for adults and youth, spanning the key points of the sequential intercept model (i.e., crisis intervention, emergency response, law enforcement diversion/deflection, pre-trial services, courts, jail, prison, re-entry services, probation, parole).
Network Structure and Objectives
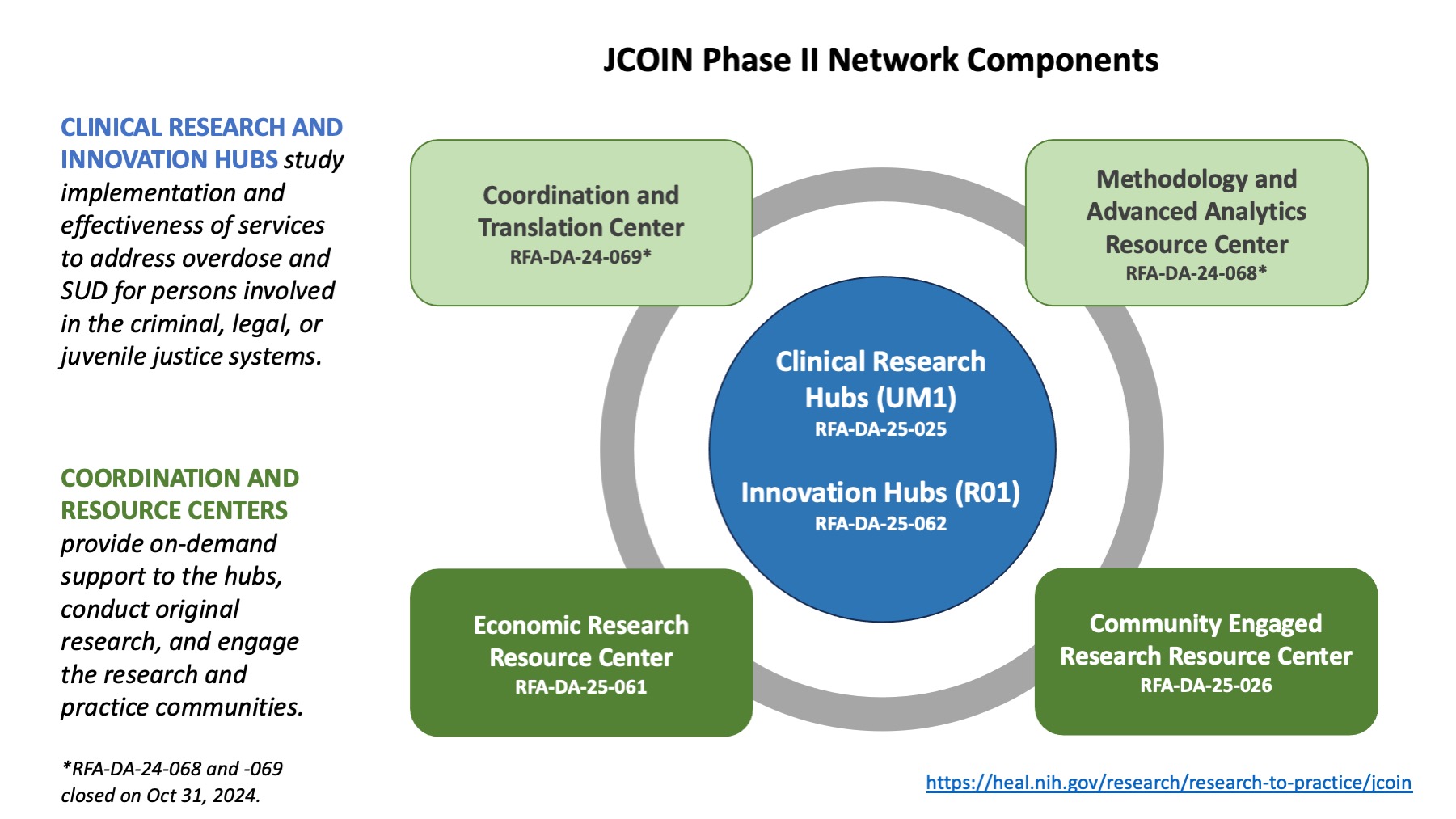
The structure of the network will include multiple research centers, working in collaboration with four complementary resource and support centers. Clinical Research Hubs (RFA-DA-25-025) are expected to conduct large multi-site studies; Innovation Hubs (RFA-DA-25-062) are intended to support smaller-scale studies. Both Clinical Research and Innovation Hubs will have the capacity to conduct collaborative pilot studies with other awardees. The CTC (RFA-DA-24-069) will facilitate collaboration among the Hubs, conduct novel dissemination and implementation research, and engage in an array of capacity building activities to engage practitioners and other key stakeholder organizations. The MAARC (RFA-DA-24-068) will provide infrastructure for data submission, data sharing, and analytic support, while conducting novel survey and modeling studies. An Economic Research Resource Center (ERRC; RFA-DA-25-061) will facilitate collaboration across Hubs on the collection, analysis, and comparison of cost data; conduct original research; and develop tools to support practitioners and decision-makers. A Community Engaged Research Resource Center (CERRC; RFA-DA-25-026) will directly engage persons with lived experience and provide additional support to the Hubs on effectively engaging affected communities in the research process.
To maximize the impact of JCOIN research, participating awardees are expected to engage individually and collectively in work that connects research to practice, incorporates patient perspectives, and considers implications for equity, scalability, and sustainability.
A visual depiction of the structure and organization of this initiative can be found at this link: https://nida.nih.gov/sites/default/files/images/JCOINPhase2.jpg.
{kind=link}
It is imperative that prospective applicants read the NOFOs associated with each of these components, in order to fully understand the intended structure and operation of the network, the scope of the component awards, and the expectations for awardees. An informational webinar for potential applicants will be held on July 25 at 2:00pm EDT. When available, a registration link and more information will be posted at: https://nida.nih.gov/news-events/meetings-events/2024/07/jcoin-phase-ii-informational-webinar-potential-applicants
This NOFO seeks applications for JCOIN Phase II Clinical Research Hubs that will conduct large multi-site clinical trials.
Scope of Activities and Purpose
The JCOIN Phase II Clinical Research Hubs will conduct clinical research and clinical trials, including implementation and hybrid implementation-effectiveness studies. Each Clinical Research Hub must propose a multi-site clinical trial with at least three sites. The goal of these studies should be to improve public health and public safety outcomes for justice-involved individuals who have SUDs or are at risk of overdose. Public health outcomes are inclusive of illicit opioid and/or stimulant use, misuse, or related overdoses and mortality among justice-involved populations. An SUD cascade or behavioral health cascade framework should be used to guide outcome selection. A behavioral health cascade framework includes screening for substance use, referral to treatment, treatment engagement and retention in behavioral and pharmacological SUD treatments. Relevant implementation outcomes such as penetration, scalability, and sustainability should also be considered.
During years 2-5, projects should plan to set aside funds to support the Hub’s engagement in at least one collaborative study with one or more other Hubs. The topic and scope of the collaborative studies will be determined post-award by the Network investigators and NIDA Project Scientist (i.e., these will be delayed onset studies). These projects will be designed to leverage opportunities that uniquely draw on the characteristics of the funded Hubs, communities, and partner agencies. Collaborative pilot studies will require NIDA Program Officer approval prior to launch.
Areas of special interest include:
- Examination of interventions, practices, or implementation strategies that are widely used, but for which there is limited evidence, especially those that occur in the early points of the sequential intercept model (e.g., law enforcement diversion and deflection strategies; crisis response team approaches).
- Studies targeting understudied justice-involved populations or settings are strongly encouraged. Examples include, but are not limited to, juvenile justice, rural settings, women, pregnant and parenting individuals, American Indian/Alaskan Native populations, concurrent multi-generational involvement in justice systems.
- Studies that, in addition to substance use treatment needs, consider and target mental and physical health comorbidities (e.g., HIV, HCV, cancer, PTSD, suicide).
- Studies that, in addition to substance use treatment needs, consider and target the complex needs of justice-involved populations, including housing, recovery supports, and employment.
- Studies that address polysubstance use, beyond opioid and stimulant use (to include alcohol and cannabis use).
- Research that addresses workforce issues, such as burnout and high turnover among correctional and behavioral health staff.
- Studies that use just-in-time or adaptive interventions for enhancing treatment outcomes.
- Research designs that can inform policy and payment models.
- Trials to improve the quality of care delivered in carceral settings.
- Study designs that support multi-jurisdictional collaborative research networks among justice agencies to study shared questions of interest using local data.
Definitions for Sites, Systems, and Service Providers:
- Clinical Research Performance Site: JCOIN Phase II Clinical Research Hub applications must propose a research project to be executed in at least three geographically distinct clinical research performance sites (i.e., three or more communities). A clinical research performance site (i.e., community) is defined as a partnership between a justice setting (e.g., jail, prison, tribal court, drug court) and one or more behavioral health or community-based service providers (e.g., hospital, SUD treatment provider, other relevant service provider). Both the justice setting and the service provider must engage with a shared population of criminal legal system-involved individuals who live or receive services in a defined geographic area (i.e., community). Each of the proposed clinical research performance sites must be geographically distinct and non-overlapping from the perspective of the population of patients engaging with services.
- Criminal Legal System/Justice System: For the purposes of this NOFO, “criminal legal system” and “justice system” are used interchangeably. They are broadly defined to include prisons, jails, tribal court, drug courts, other problem-solving courts, civil commitment courts, law enforcement diversion and deflection programs (e.g., crisis intervention, emergency response teams), transitions to secure settings from communities (e.g., central intake facilities), transitions from secure settings to communities (i.e., re-entry), and community corrections (probation and parole). Juvenile justice and child welfare systems are also permitted. Applicants may focus on one or more intercept points. A key area of interest is testing models to provide evidence-based treatment, including treatment for co-occurring mental health and SUD, to individuals at various points in the criminal justice sequential intercept model.
- Community-Based/Behavioral Health Services: For the purposes of this NOFO, a community-based or behavioral health service provider is inclusive of any organization or setting where a patient may engage with medical or behavioral health services that address SUD treatment, overdose prevention, or related treatment and other service needs. This includes, but is not limited to contracted medical and behavioral health care providers, HIV service providers, Federally Qualified Health Centers (FQHCs), integrated primary care and behavioral health clinics, office-based opioid agonist treatment providers, harm reduction sites, housing providers, methadone clinics, SUD treatment programs, etc.
Research Design and Outcome Selection
Proposed research projects for JCOIN Phase II Clinical Research Hubs are required to leverage implementation, and hybrid implementation-effectiveness designs.
Hybrid implementation-effectiveness study designs may examine FDA-approved medications, evidence-based behavioral interventions and digital therapeutics (including adaptations and refinements), and comprehensive, patient-centered intervention packages. Key outcomes of interest include treatment engagement and retention, remission, relapse, overdose, overdose and all-cause mortality, and recidivism. Indicators of reduced opioid, stimulant and other substance use, along with criminal activity, and behavior while in custody are also relevant outcomes. Applicants are strongly encouraged to utilize an SUD or behavioral health care cascade framework as a guide for selecting outcomes. Public safety and public health outcomes should be included. Applicants are strongly encouraged to include follow-up periods of one year or longer if feasible.
Rigorous economic evaluations, especially cost-effectiveness analyses, such as those following the recommendations of the Second Panel on Cost-Effectiveness in Health and Medicine, are encouraged to be included as part of the study design. Economic evaluations that consider relevant economic outcomes of proposed interventions from a societal perspective (e.g., costs of treatment, crime, etc.) are especially encouraged. All projects should include a cost component and should plan to collaborate with the JCOIN Phase II ERRC. As part of collaboration with the ERRC, Clinical Research Hubs are expected to engage in a needs assessment within the first 4 months after award. The ERRC will assist the Hubs in identifying opportunities, measures, and methods for addressing economic research questions.
Clients, patients, individuals with lived experience and other key stakeholder groups are the consumers of the interventions developed by NIH supported clinical trial research. Meaningful engagement and collaboration with these partners throughout the research process, including research design, conduct, and dissemination of study findings, have the potential to improve the quality of care, maximize implementation, and sustain utilization of these interventions. Hence, all projects must also include a Stakeholder Engagement and Dissemination Plan, which describes how the research team will meaningfully engage justice and behavioral health partners as well as the intended recipients of the proposed intervention. These plans should be explicit with regard to engagement prior to study launch, during study execution, and plans for meaningful sharing of results with relevant stakeholders. Applicants should leverage these perspectives to inform best practices for disseminating research findings to target audiences beyond the research community.
Example Research Questions
Effectiveness questions can be addressed by the Clinical Research Hubs. However, applications must also address relevant implementation science questions. Examples of effectiveness questions include, but are not limited to:
- How can technology and digital therapeutics be employed to improve outcomes for individuals with SUDs in carceral and community settings, as well as facilitating transitions between settings?
- How can just-in-time or adaptive interventions (e.g., Sequential Multiple Assignment Randomized Trials and Multi-phase Optimization Strategy designs) be used to enhance treatment outcomes?
- What are effective interventions models for addressing co-morbid mental health and substance use outcomes for individuals with criminal legal system involvement?
- Are emerging strategies such as law enforcement deflection/diversion, crisis response models, or civil commitments effective at engaging and retaining individuals in evidence-based substance use treatment?
- How effective are evidence-based SUD treatments at meeting the needs of understudied justice-involved populations?
Examples of implementation questions include, but are not limited to:
- What are the best implementation strategies for improving collaboration between community health and justice systems to increase engagement and retention in addiction treatment?
- What implementation strategies are effective in facilitating the development of data-driven learning healthcare approaches in justice-public health collaborations?
- What is the role of technology as an implementation tool for facilitating collaborative relationships between public health and public safety?
- What implementation strategies are effective in addressing co-occurring mental health and substance use issues among criminal legal system involved populations?
- What implementation strategies are effective in addressing social determinants of health (e.g., housing, employment) and substance use for individuals with criminal legal system involvement?
- What implementation models can support the development of trans-organizational learning healthcare systems in public health and public safety partnerships?
Examples of hybrid implementation-effectiveness questions include, but are not limited to:
- What implementation strategies are most effective at facilitating the adoption of technology-driven interventions to improve patient- and system-level outcomes?
- How can multi-level interventions be leveraged to enhance treatment engagement and cross-system data sharing?
- What are the best models for reducing stigma about medications for opioid use disorders (MOUDs) among justice system personnel, and how do they affect treatment and public safety outcomes for individuals in the criminal legal system?
- How does delivery of MOUD in carceral settings affect correctional staff morale, and system level outcomes (e.g., facility safety, staff turnover)?
- What are the impacts of MOUDs delivered in carceral settings on outcomes during incarceration? What implementation strategies can best support the reach and impact of these medications? What are the optimal procedures and timing of delivering MOUDs during periods of incarceration that exceed 1 year?
As appropriate to study design and aims, applicants should plan to use the core measures developed for JCOIN Phase I available at: https://nida.nih.gov/research/nida-research-programs-activities/justice-system-research. Where appropriate, successful applicants will be encouraged to collect common organizational, environmental or other contextual data in addition to patient-level common measures.
Network Participation: The JCOIN Phase II Clinical Research Hub investigators are expected to participate in monthly Steering Committee (SC) or work group calls with the other Hubs and resource and support centers. Hubs are also required to participate in one needs assessment meeting with the Economics Research Resource Center within the first 4 months after award, and one needs assessment meeting with the CERRC within 12 months after award. One annual in-person meeting for the Network, in the Bethesda, MD area, to include key project staff for each Hub (likely 3-5 team members), should be anticipated. During the first year, Hub awardees will collaborate with other Hubs and the MAARC to identify a set of common measures to be used, as relevant, across studies and determine policies and processes for data sharing and collaborative analysis.Hub awardees should anticipate upload of clinical trial and other study data to the JCOIN Data Commons at regular intervals. All participants in the Network will have opportunities to collaborate on emergent, shared priorities.
Applications Not Responsive to this NOFO
The following types of studies are not responsive to this NOFO and will not be reviewed:
- Clinical Research Hubs that do not emphasize treatment of illicit opioid and/or stimulant use or misuse among justice-involved individuals. Opioid and/or stimulant-relevant outcomes must be included.
- Research sites with communities outside the US and its territories.
- Clinical Research Hubs that do not include an implementation science component.
- Applications that do not propose conducting research in at least three communities.
- Applications that do not include letters of support from proposed justice settings and community-based or behavioral health service providers, as relevant to the study design.
- Applications that do not include one or more senior-level collaborators from both justice and community-based and behavioral health providers, as relevant to the study design.
Pre-Application Consultation: Potential applicants are strongly encouraged to consult with NIDA program staff early in the application development process. This early contact will provide an opportunity to discuss and clarify NIH policies and guidelines, including the scope of the project relative to the intent of this NOFO. See Scientific/Program Contacts in Section VII.
Special Considerations: NIDA applicants are strongly encouraged to review the guidelines and adhere to the requirements applicable to their research listed in the Special Considerations for NIDA Funding Opportunities and Awards. Upon award, these considerations will be included in the Notice of Grant Award.
Plan for Enhancing Diverse Perspectives (PEDP)
The NIH recognizes that teams comprised of investigators with diverse perspectives working together and capitalizing on innovative ideas and distinct viewpoints outperform homogeneous teams. There are many benefits that flow from a scientific workforce rich with diverse perspectives, including: fostering scientific innovation, enhancing global competitiveness, contributing to robust learning environments, improving the quality of the research, advancing the likelihood that underserved populations participate in, and benefit from research, and enhancing public trust.
To support the best science, the NIH encourages inclusivity in research guided by the consideration of diverse perspectives. Broadly, diverse perspectives can include but are not limited to the educational background and scientific expertise of the people who perform the research; the populations who participate as human subjects in research studies; and the places where research is done.
This NOFO requires a Plan for Enhancing Diverse Perspectives (PEDP), which will be assessed as part of the scientific and technical peer review evaluation. Assessment of applications containing a PEDP are based on the scientific and technical merit of the proposed project. Consistent with federal law, the race, ethnicity, or sex of a researcher, award participant, or trainee will not be considered during the application review process or when making funding decisions. Applications that fail to include a PEDP will be considered incomplete and will be administratively withdrawn before review.
The PEDP will be submitted as Other Project Information as an attachment (see Section IV). Applicants are strongly encouraged to read the NOFO instructions carefully and view the available PEDP guidance materials.
HEAL PI Meeting Attendance: The NIH HEAL Initiative will require a high level of coordination and sharing between investigators. It is expected that NIH HEAL Initiative awardees will cooperate and coordinate their activities after awards are made by participating in Program Director/Principal Investigator (PD/PI) meetings, including an annual HEAL Investigators Meeting, as well as other activities.
The NIH HEAL Initiative will require a high level of coordination and sharing between investigators. It is expected that NIH HEAL Initiative awardees will cooperate and coordinate their activities after awards are made by participating in Program Director/Principal Investigator (PD/PI) meetings, including an annual HEAL Investigators Meeting, as well as other activities.
Clinical Trial Accrual: This NOFO will support applications that include a series of milestones for completion of the clinical trial and provide contingency plans to proactively confront potential delays or disturbances in attaining the milestones. Continuation of the award is conditional upon satisfactory progress, availability of funds, and scientific priorities of the HEAL Initiative. If, at any time, recruitment falls significantly below the projected milestones for recruitment, NIH will consider ending support and negotiating an orderly phase-out of the award. NIH retains the option of periodic external peer review of progress. NIH program staff will closely monitor progress at all stages for milestones, accrual, and safety.
Applicants are reminded that NIH requires all individuals listed on the R&R Senior/Key Person Profile (Expanded) Form to have an eRA Commons username (Commons ID). This includes non-academic collaborators meeting the definition of Senior/Key Personnel. See NOT-OD-21-109 and NOT-OD-24-042. Options for obtaining an eRA Commons username (Commons ID) for a senior/key person who isn’t affiliated with a registered organization can be found here.
See Section VIII. Other Information for award authorities and regulations.
Investigators proposing NIH-defined clinical trials may refer to the Research Methods Resources website for information about developing statistical methods and study designs.
Cooperative Agreement: A financial assistance mechanism used when there will be substantial Federal scientific or programmatic involvement. Substantial involvement means that, after award, NIH scientific or program staff will assist, guide, coordinate, or participate in project activities. See Section VI.2 for additional information about the substantial involvement for this NOFO.
The OER Glossary and the How to Apply - Application Guide provides details on these application types. Only those application types listed here are allowed for this NOFO.
Required: Only accepting applications that propose clinical trial(s).
NIDA intends to commit $14,000,000 in FY 2025 to fund 8-10 awards.
Direct costs are limited to $5,000,000 over the 5-year project period, with no more than $1,000,000 in direct costs allowed in any single year.
The total project period for an application submitted may not exceed five years.
NIH grants policies as described in the NIH Grants Policy Statement will apply to the applications submitted and awards made from this NOFO.
1. Eligible Applicants
All organizations administering an eligible parent award may apply for a supplement under this NOFO.
Higher Education Institutions
- Public/State Controlled Institutions of Higher Education
- Private Institutions of Higher Education
The following types of Higher Education Institutions are always encouraged to apply for NIH support as Public or Private Institutions of Higher Education:
- Hispanic-serving Institutions
- Historically Black Colleges and Universities (HBCUs)
- Tribally Controlled Colleges and Universities (TCCUs)
- Alaska Native and Native Hawaiian Serving Institutions
- Asian American Native American Pacific Islander Serving Institutions (AANAPISIs)
Nonprofits Other Than Institutions of Higher Education
- Nonprofits with 501(c)(3) IRS Status (Other than Institutions of Higher Education)
- Nonprofits without 501(c)(3) IRS Status (Other than Institutions of Higher Education)
For-Profit Organizations
- Small Businesses
- For-Profit Organizations (Other than Small Businesses)
Local Governments
- State Governments
- County Governments
- City or Township Governments
- Special District Governments
- Indian/Native American Tribal Governments (Federally Recognized)
- Indian/Native American Tribal Governments (Other than Federally Recognized)
Federal Government
- Eligible Agencies of the Federal Government
- U.S. Territory or Possession
Other
- Independent School Districts
- Public Housing Authorities/Indian Housing Authorities
- Native American Tribal Organizations (other than Federally recognized tribal governments)
- Faith-based or Community-based Organizations
- Regional Organizations
Non-domestic (non-U.S.) Entities (Foreign Organizations) are not eligible to apply.
Non-domestic (non-U.S.) components of U.S. Organizations are not eligible to apply.
Foreign components, as defined in the NIH Grants Policy Statement, are allowed.
Applicant Organizations
Applicant organizations must complete and maintain the following registrations as described in the How to Apply - Application Guide to be eligible to apply for or receive an award. All registrations must be completed prior to the application being submitted. Registration can take 6 weeks or more, so applicants should begin the registration process as soon as possible. Failure to complete registrations in advance of a due date is not a valid reason for a late submission, please reference NIH Grants Policy Statement Section 2.3.9.2 Electronically Submitted Applications for additional information.
- System for Award Management (SAM) – Applicants must complete and maintain an active registration, which requires renewal at least annually. The renewal process may require as much time as the initial registration. SAM registration includes the assignment of a Commercial and Government Entity (CAGE) Code for domestic organizations which have not already been assigned a CAGE Code.
- NATO Commercial and Government Entity (NCAGE) Code – Foreign organizations must obtain an NCAGE code (in lieu of a CAGE code) in order to register in SAM.
- Unique Entity Identifier (UEI) - A UEI is issued as part of the SAM.gov registration process. The same UEI must be used for all registrations, as well as on the grant application.
- eRA Commons - Once the unique organization identifier is established, organizations can register with eRA Commons in tandem with completing their Grants.gov registration; all registrations must be in place by time of submission. eRA Commons requires organizations to identify at least one Signing Official (SO) and at least one Program Director/Principal Investigator (PD/PI) account in order to submit an application.
- Grants.gov – Applicants must have an active SAM registration in order to complete the Grants.gov registration.
Program Directors/Principal Investigators (PD(s)/PI(s))
All PD(s)/PI(s) must have an eRA Commons account. PD(s)/PI(s) should work with their organizational officials to either create a new account or to affiliate their existing account with the applicant organization in eRA Commons. If the PD/PI is also the organizational Signing Official, they must have two distinct eRA Commons accounts, one for each role. Obtaining an eRA Commons account can take up to 2 weeks.
Any individual(s) with the skills, knowledge, and resources necessary to carry out the proposed research as the Program Director(s)/Principal Investigator(s) (PD(s)/PI(s)) is invited to work with their organization to develop an application for support. Individuals from diverse backgrounds, including underrepresented racial and ethnic groups, individuals with disabilities, and women are always encouraged to apply for NIH support. See, Reminder: Notice of NIH's Encouragement of Applications Supporting Individuals from Underrepresented Ethnic and Racial Groups as well as Individuals with Disabilities, NOT-OD-22-019.
For institutions/organizations proposing multiple PDs/PIs, visit the Multiple Program Director/Principal Investigator Policy and submission details in the Senior/Key Person Profile (Expanded) Component of the How to Apply - Application Guide.
2. Cost Sharing
This NOFO does not require cost sharing as defined in the NIH Grants Policy Statement Section 1.2 Definition of Terms.
3. Additional Information on Eligibility
Number of Applications
Applicant organizations may submit more than one application, provided that each application is scientifically distinct.
The NIH will not accept duplicate or highly overlapping applications under review at the same time, per NIH Grants Policy Statement Section 2.3.7.4 Submission of Resubmission Application. This means that the NIH will not accept:
- A new (A0) application that is submitted before issuance of the summary statement from the review of an overlapping new (A0) or resubmission (A1) application.
- A resubmission (A1) application that is submitted before issuance of the summary statement from the review of the previous new (A0) application.
- An application that has substantial overlap with another application pending appeal of initial peer review (see NIH Grants Policy Statement 2.3.9.4 Similar, Essentially Identical, or Identical Applications).
1. Requesting an Application Package
The application forms package specific to this opportunity must be accessed through ASSIST, Grants.gov Workspace or an institutional system-to-system solution. Links to apply using ASSIST or Grants.gov Workspace are available in Part 1 of this NOFO. See your administrative office for instructions if you plan to use an institutional system-to-system solution.
2. Content and Form of Application Submission
It is critical that applicants follow the instructions in the Research (R) Instructions in the How to Apply - Application Guide except where instructed in this notice of funding opportunity to do otherwise. Conformance to the requirements in the How to Apply - Application Guide is required and strictly enforced. Applications that are out of compliance with these instructions may be delayed or not accepted for review.
Letter of Intent
Although a letter of intent is not required, is not binding, and does not enter into the review of a subsequent application, the information that it contains allows IC staff to estimate the potential review workload and plan the review.
By the date listed in Part 1. Overview Information, prospective applicants are asked to submit a letter of intent that includes the following information:
- Descriptive title of proposed activity
- Name(s), address(es), and telephone number(s) of the PD(s)/PI(s)
- Names of other key personnel
- Participating institution(s)
- Number and title of this funding opportunity
The letter of intent should be sent to: [email protected].
All page limitations described in the How to Apply – Application Guide and the Table of Page Limits must be followed.
The following section supplements the instructions found in the How to Apply – Application Guide and should be used for preparing an application to this NOFO.
All instructions in the How to Apply - Application Guide must be followed.
All instructions in the How to Apply - Application Guide must be followed, with the following additional instructions:
- Data should be presented on the nature, severity, and trends in opioid and/or stimulant use, opioid and/or stimulant related morbidity and mortality, or other opioid and/or stimulant-related outcomes for the targeted communities. If available, data on opioid and/or stimulant use in the targeted justice setting specifically should be presented, though not required. This may be presented broadly for the pool of sites and/or specifically for each proposed site, depending on study design.
- Capacity to recruit additional sites, if needed, should be described.
- As noted in the Research Strategy Instructions, for each proposed community, letters of support from both the (a) targeted justice entity(ies) and (b) community-based or behavioral health service provider entity(ies) should be provided, as applicable to the proposed study. If a study design proposes recruiting sites as part of a study design, strong justifications demonstrating feasibility of recruitment (e.g., letters of support from a state government official overseeing a system with multiple potential sites) and a strong justification for the selection of this strategy must be included.
All instructions in the How to Apply - Application Guide must be followed, with the following additional instructions:
Other Attachments:
Stakeholder Engagement and Dissemination Plan (Required – 3 page maximum)
All projects must also include a plan for meaningfully engaging justice and behavioral health partners as well as individuals with lived experience relevant to the research project. These plans should be explicit with regard to engagement prior to study launch, during study execution, and plans for meaningful sharing of results with relevant stakeholders. Dissemination strategies should include at least one presentation per year in years 3-5 at a practitioner conference.
Plan for Enhancing Diverse Perspectives (PEDP)
- In an "Other Attachment" entitled "Plan for Enhancing Diverse Perspectives," all applicants must include a summary of actionable strategies to advance the scientific and technical merit of the proposed project through expanded inclusivity.
- Applicants should align their proposed strategies for PEDP with the research strategy section, providing a holistic and integrated view of how enhancing diverse perspectives and inclusivity are buoyed throughout the application.
- The PEDP will vary depending on the scientific aims, expertise required, the environment and performance site(s), as well as how the project aims are structured.
- The PEDP may be no more than 2 pages in length and should include:
- Actionable strategies using defined approaches for the inclusion of diverse perspectives in the project;
- Description of how the PEDP will advance the scientific and technical merit of the proposed project;
- Anticipated timeline of proposed PEDP activities;
- Evaluation methods for assessing the progress and success of PEDP activities.
Examples of items that advance inclusivity in research and may be appropriate for a PEDP can include, but are not limited to:
- Partnerships with different types of institutions and organizations (e.g., research-intensive; undergraduate-focused; HBCUs; emerging research institutions; community-based organizations).
- Project frameworks that enable communities and researchers to work collaboratively as equal partners in all phases of the research process.
- Outreach and planned engagement activities to enhance recruitment of individuals from diverse groups as human subjects in clinical trials, including those from underrepresented backgrounds.
- Description of planned partnerships that may enhance geographic and regional diversity.
- Outreach and recruiting activities intended to diversify the pool of applicants for research training programs, such as outreach to prospective applicants from groups underrepresented in the biomedical sciences, for example, individuals from underrepresented racial and ethnic groups, those with disabilities, those from disadvantaged backgrounds, and women.
- Plans to utilize the project infrastructure (i.e., research and structure) to enhance the research environment and support career-advancing opportunities for junior, early- and mid-career researchers.
- Transdisciplinary research projects and collaborations among researchers from fields beyond the biological sciences, such as physics, engineering, mathematics, computational biology, computer and data sciences, as well as bioethics.
Examples of items that are not appropriate in a PEDP include, but are not limited to:
- Selection or hiring of personnel for a research team based on their race, ethnicity, or sex.
- A training or mentorship program limited to certain researchers based on their race, ethnicity, or sex.
For further information on the Plan for Enhancing Diverse Perspectives (PEDP), please see PEDP guidance materials.
All instructions in the How to Apply - Application Guide must be followed, with the following additional instructions:
Biosketches should describe Senior/Key Personnel recent experience and participation in randomized clinical trials, preferably of a multi-site nature. Applicants are expected to provide evidence of their unique strengths, accomplishments and capabilities to contribute to shared activities across the JCOIN network. Applicants should provide evidence of expertise in the conduct of clinical trials, particularly cooperative, pragmatic, randomized clinical trials. Persons responsible for participant recruitment, enrollment, data collection and data management should be shown to have extensive experience and high qualifications.
Biosketches must be included for one or more senior leaders from (a) a justice setting and (b) a community-based or behavioral health treatment provider, as relevant to the proposed study. Senior leaders do not have to be from one of the targeted communities if not appropriate for the study design, but should have relevant expertise and demonstrate the ability to provide guidance to the research team on pragmatic and practice-related issues relevant to research in the targeted setting. Applicants are reminded that NIH requires all individuals listed on the R&R Senior/Key Person Profile (Expanded) Form to have an eRA Commons username (Commons ID). This includes non-academic collaborators meeting the definition of Senior/Key Personnel. See NOT-OD-21-109 and NOT-OD-24-042. Options for obtaining an eRA Commons username (Commons ID) for a senior/key person who isn’t affiliated with a registered organization can be found here.
PD/PIs, senior investigators, and other investigators with substantial time commitments to JCOIN should expect to actively participate in a wide variety of network activities, including, but not limited to: providing mentorship to participants in the CTC Research Education Core (see RFA-DA-24-069 for more detail), participating in reviews of network publications, actively engaging in harmonization activities, making data from their study available to others in a timely manner, serving as a reviewer for CTC Rapid Response and Pilot Research Project applications (see RFA-DA-24-069 for more detail), participating in cross-hub cost-effectiveness or other economic analyses as coordinated by the ERRC, actively contributing to activities led by the CERRC to ensure that principles of justice, equity, diversity and inclusion are upheld at each Hub, and engaging with other investigators and the NIDA Science Officer in cross-hub research projects.
R&R Budget
All instructions in the How to Apply - Application Guide must be followed, with the following additional instructions:
Requirements for Senior Personnel:
PIs must commit two (2.0) person-months effort annually on the award over the entire period of support. In a multi-PI application, at least one PD/PI must commit a minimum of 2.0 person-months annually over the life of the grant award.
In addition to executing the proposed protocol, applicants will be expected to participate in network activities. Time should be budgeted to participate in such activities.
Applicants are encouraged to include support for individuals with lived experience and other relevant stakeholders. Budgetary support might include allowable salary support or honorarium, travel, and per diem costs. If applications have not selected individuals for these roles, it is appropriate to set aside a number of slots to fill in after the stakeholder needs have been established based on the research project.
PEDP implementation costs:
Applicants may include allowable costs associated with PEDP implementation (as outlined in the Grants Policy Statement section 7: https://grants.nih.gov/grants/policy/nihgps/html5/section_7/7.1_general.htm).
Travel for annual meetings:
Applicants should budget for three to five project staff to attend one in-person JCOIN Steering Committee (SC) meeting per year; assume each meeting is 2 days and is in Bethesda Maryland. Project leadership should also anticipate attendance at monthly virtual SC meetings for the duration of the award. One Hub PI is expected to attend the annual HEAL Scientific Meeting each year – for budget purposes, assume this is a 2-day meeting in the Washington DC area.
Collaborative Projects:
Applicants must budget $100,000/year (direct costs) during years 2-5 for collaborative projects.
Note: Beginning in 2026, all NIH-funded publications must be open access immediately. Applicants are encouraged to budget for publication fees, if needed to comply with the new NIH policy.
R&R Subaward Budget
All instructions in the How to Apply - Application Guide must be followed.
All instructions in the How to Apply - Application Guide must be followed.
All instructions in the How to Apply - Application Guide must be followed, with the following additional instructions:
Research Strategy:
Each JCOIN Phase II Clinical Research Hub should propose a multi-site research project. All proposed projects must engage three or more performance sites (i.e., communities). The number of sites engaged should be appropriate to the goals of the proposed study and the study should be adequately powered to detect proposed outcomes.
The research strategy section should be organized as follows:
Section A: Research Strategy:
Applicants are requested to develop and propose a research concept that lays out a theoretically grounded, hypothesis-driven study design to address gaps in the continuum of care for individuals involved in the criminal legal system. Applications must advance delivering or optimizing evidence-based interventions to prevent and treat opioid and/or stimulant use, misuse, and addiction in criminal legal system involved populations. Applications must generate novel information about how to improve collaborations between justice and community-based/behavioral health providers to improve public health and public safety outcomes.
Applications should involve stakeholders and clinical research performance sites from both justice settings and community-based or behavioral health service providers. A focus on community-based settings is inclusive of transitions from secure settings and communities, so may include, for example, a focus on continuing medications during entry into secure settings and resuming or maintaining medications during community re-entry.
Applicants are encouraged to consider relevant issues such as comorbid mental health and physical health issues, polysubstance use, social determinants of health, trauma-informed approaches, etc. Designs may engage a variety of community-based providers who provide services targeting common comorbid issues. Primary outcomes, however, must include opioid and/or stimulant-relevant outcomes.
Applications should provide a detailed overview of the research design and sample of the proposed study. This overview should include:
- A detailed description of the proposed research project, including a clear specification of the proposed criminal legal system target and the community-based or behavioral health provider, as relevant to the proposed study.
- A rigorous study design, appropriate to the goals of the proposed research. Proposed research projects are required to leverage implementation, and hybrid implementation-effectiveness designs.
- Description of study outcomes. As described above, study outcomes should include relevant opioid and/or stimulant, public health, and public safety outcomes. Applicants are strongly encouraged to define outcomes across a full continuum of care, using standardized measures that leverage the concept of a behavioral health services cascade and/or SUD cascade. Economic outcomes should also be included.
- A strong justification for the selected follow-up period. Applicants are strongly encouraged to plan for follow-ups for one year or longer.
- As appropriate to study design and aims, applicants should plan to use the core measures developed for JCOIN Phase I available at: https://nida.nih.gov/research/nida-research-programs-activities/justice-system-research.
- A brief description of proposed clinical performance sites, including: (1) Detailed plans for ensuring high rates of recruitment and retention; and (2) Justification of the selected number of sites including power analyses appropriate to targeted outcomes and study design. Please see notes below for additional guidance regarding proposed clinical performance sites.
- Potential sustainability and scalability of the proposed intervention must be addressed. The research project should be of sufficient priority to these stakeholders that there is potential for positive findings from the study to be sustainably incorporated into standard practice after the study concludes.
- Generalizability of these sites to other settings must be discussed.
Selection and Justification of Proposed Clinical Research Performance Sites:
A minimum of three clinical research performance sites are required. Letters of Support and required details for each research performance site should be provided in Project/Performance Site Location section. The following guidelines should be followed with respect to selecting clinical performance sites:
- A clinical research performance site is defined as a geographically distinct community, and must include: (a) one or more partners from the targeted justice setting in the community, and (b) one or more community-based or behavioral health service providers, as relevant to the proposed project. Definitions of the scope of the justice system and community-based service providers are outlined in the Scope of Activities and Purpose section of this announcement.
- If there is any ambiguity with regard to the geographic distinctness of the proposed clinical research performance sites, applicants must provide a clear justification for their site selection approach.
- Although a minimum of three clinical research performance sites must be engaged, the actual number of clinical performance sites should be justified scientifically based on power analyses appropriate to the design and outcomes of interest in the proposed study.
- In general, it is anticipated that in all three performance sites, criminal legal system settings will be of the same general type (e.g., jails), but applicants can make a case for other designs with a compelling justification.
- In general, it is expected that applicants will be able to pre-specify their expected clinical research performance sites. If there is a compelling reason why this cannot or should not be done, applicants should provide similar detail to that described below regarding potential sites and what approach will be used in ultimately selecting sites.
- Additional detail should be included on planned performance sites as detailed in the SF424(R&R) Project/Performance Site Locations
Section B: Clinical Research Hub Collaboration Capacity
The research strategy section should also include a general discussion of the JCOIN Phase II Clinical Research Hub’s capacities to engage with the rest of the JCOIN network, including capacity to:
- Participate in data harmonization and other collaborative efforts within the network.
- Commit to provide the MAARC with timely, accurate data uploads.
- Engage with the ERRC to identify potential opportunities for addressing economic research questions.
- Engage with the CERRC to ensure that principles of justice, equity, diversity, and inclusion are upheld.
- Contribute unique expertise and research capacity to the network.
- Demonstrate a track record of collaboration in similar multi-site and multi-center efforts.
- If multiple organizations will collaborate as part of the proposed Clinical Research Hub, a plan for collaboration within the Hub must be presented as well.
- PI and Partners will be expected to participate in monthly SC Calls.
Letters of Support: For each proposed community, letters of support from both the (a) targeted justice entity(ies) and (b) community-based/behavioral health service provider entity(ies) must be provided. If a study design proposes recruiting sites as part of a study design, strong justifications demonstrating feasibility of recruitment (e.g., letters of support from a state government official overseeing a system with multiple potential sites) and a strong justification for the selection of this strategy must be included.
Resource Sharing Plan:
Individuals are required to comply with the instructions for the Resource Sharing Plans as provided in the How to Apply - Application Guide.
Other Plan(s):
Note: Effective for due dates on or after January 25, 2023, the Data Management and Sharing Plan will be attached in the Other Plan(s) attachment in FORMS-H application forms packages.
All instructions in the How to Apply - Application Guide must be followed, with the following additional instructions:
- All applicants planning research (funded or conducted in whole or in part by NIH) that results in the generation of scientific data are required to comply with the instructions for the Data Management and Sharing Plan. All applications, regardless of the amount of direct costs requested for any one year, must address a Data Management and Sharing Plan.
The HEAL Initiative has additional requirements that must be addressed in the Data management and Sharing plan. All HEAL-generated data must be shared through the HEAL Initiative Data Ecosystem following HEAL’s compliance guidance (https://heal.nih.gov/data/complying-heal-data-sharing-policy). Specifically, HEAL applicants must include:
- Plans to submit data and metadata (and code, if applicable) to a HEAL-Compliant data repository (https://www.healdatafair.org/resources/guidance/selection) and follow requirements of the selected repository
- Plans to register your study with the HEAL platform within one year of award (https://heal.github.io/platform-documentation/study-registration/)
- Plans to submit HEAL-defined study-level metadata within one year of award (https://github.com/HEAL/heal-metadata-schemas/blob/main/for-investigators-how-to/study-level-metadata-fields/study-metadata-schema-for-humans.pdf) and https://heal.github.io/platform-documentation/slmd_submission/.
- HEAL pain clinical studies must include plan to use HEAL core Common Data Elements (https://heal.nih.gov/data/common-data-elements). HEAL Initiative clinical studies that are using copyrighted questionaries are required to obtain licenses for use prior to initiating data collection. Licenses must be shared with the HEAL CDE team and the program officer prior to use of copyrighted materials.
- To the extent possible, all other (non-pain) HEAL studies conducting clinical trials or research involving human subject are expected to use questionnaires by the HEAL Clinical Data Elements (CDE) Program (https://heal.nih.gov/data/common-data-elements) if applicable and relevant to their research.
- Studies using CDEs, regardless of whether they are part of the HEAL repository, will be required to report which questionnaires are being used.
- To the extent possible, HEAL awardees are expected to integrate broad data sharing consent language into their informed consent forms.
HEAL has developed additional details and resources to fulfill these requirements (https://www.healdatafair.org/resources/road-map).
HEAL Public Access and Data Sharing Policy:
NIH intends to maximize the impact of HEAL Initiative-supported projects through broad and rapid data sharing and immediate access to publications (https://heal.nih.gov/about/public-access-data). Guidelines for complying with the HEAL Public Access and Data Sharing Policy can be found at https://heal.nih.gov/data/complying-heal-data-sharing-policy. Resources and tools to assist with data related activities can be found at https://www.healdatafair.org/. For more detail and specific data sharing requirements, see Section 4. Other plans.
Publications resulting from NIH HEAL Initiative funded studies must be immediately publicly available upon publication.
- For manuscripts published in journals that are not immediately open access, authors should arrange with journals in advance to pay for immediate open access
- Costs to ensure manuscripts are immediately publicly available upon publication should be included in budget requests
Only limited Appendix materials are allowed. Follow all instructions for the Appendix as described in the How to Apply - Application Guide.
When involving human subjects research, clinical research, and/or NIH-defined clinical trials (and when applicable, clinical trials research experience) follow all instructions for the PHS Human Subjects and Clinical Trials Information form in the How to Apply - Application Guide, with the following additional instructions:
If you answered “Yes” to the question “Are Human Subjects Involved?” on the R&R Other Project Information form, you must include at least one human subjects study record using the Study Record: PHS Human Subjects and Clinical Trials Information form or Delayed Onset Study record.
Study Record: PHS Human Subjects and Clinical Trials Information
All instructions in the How to Apply - Application Guide must be followed.
Delayed Onset Study
Note: Delayed onset does NOT apply to a study that can be described but will not start immediately (i.e., delayed start). All instructions in the How to Apply - Application Guide must be followed.
All instructions in the How to Apply - Application Guide must be followed.
3. Unique Entity Identifier and System for Award Management (SAM)
See Part 2. Section III.1 for information regarding the requirement for obtaining a unique entity identifier and for completing and maintaining active registrations in System for Award Management (SAM), NATO Commercial and Government Entity (NCAGE) Code (if applicable), eRA Commons, and Grants.gov
Part I. contains information about Key Dates and times. Applicants are encouraged to submit applications before the due date to ensure they have time to make any application corrections that might be necessary for successful submission. When a submission date falls on a weekend or Federal holiday, the application deadline is automatically extended to the next business day.
Organizations must submit applications to Grants.gov (the online portal to find and apply for grants across all Federal agencies). Applicants must then complete the submission process by tracking the status of the application in the eRA Commons, NIH’s electronic system for grants administration. NIH and Grants.gov systems check the application against many of the application instructions upon submission. Errors must be corrected and a changed/corrected application must be submitted to Grants.gov on or before the application due date and time. If a Changed/Corrected application is submitted after the deadline, the application will be considered late. Applications that miss the due date and time are subjected to the NIH Grants Policy Statement Section 2.3.9.2 Electronically Submitted Applications.
Applicants are responsible for viewing their application before the due date in the eRA Commons to ensure accurate and successful submission.
Information on the submission process and a definition of on-time submission are provided in the How to Apply – Application Guide.
5. Intergovernmental Review (E.O. 12372)
This initiative is not subject to intergovernmental review.
All NIH awards are subject to the terms and conditions, cost principles, and other considerations described in the NIH Grants Policy Statement.
Pre-award costs are allowable only as described in the NIH Grants Policy Statement Section 7.9.1 Selected Items of Cost.
Applications must be submitted electronically following the instructions described in the How to Apply - Application Guide. Paper applications will not be accepted.
Applicants must complete all required registrations before the application due date. Section III. Eligibility Information contains information about registration.
For assistance with your electronic application or for more information on the electronic submission process, visit How to Apply – Application Guide. If you encounter a system issue beyond your control that threatens your ability to complete the submission process on-time, you must follow the Dealing with System Issues guidance. For assistance with application submission, contact the Application Submission Contacts in Section VII.
Important reminders:
All PD(s)/PI(s) must include their eRA Commons ID in the Credential field of the Senior/Key Person Profile form. Failure to register in the Commons and to include a valid PD/PI Commons ID in the credential field will prevent the successful submission of an electronic application to NIH. See Section III of this NOFO for information on registration requirements.
The applicant organization must ensure that the unique entity identifier provided on the application is the same identifier used in the organization’s profile in the eRA Commons and for the System for Award Management. Additional information may be found in the How to Apply - Application Guide.
See more tips for avoiding common errors.
Upon receipt, applications will be evaluated for completeness and compliance with application instructions by the Center for Scientific Review and responsiveness by NIDA, NIH. Applications that are incomplete, non-compliant and/or nonresponsive will not be reviewed.
Applications must include annual milestones. Applications that fail to include annual milestones will be considered incomplete and will be withdrawn.
Applications must include a PEDP submitted as Other Project Information as an attachment. Applications that fail to include a PEDP will be considered incomplete and will be administratively withdrawn before review.
Applicants are required to follow the instructions for post-submission materials, as described in the policy
1. Criteria
Only the review criteria described below will be considered in the review process. Applications submitted to the NIH in support of the NIH mission are evaluated for scientific and technical merit through the NIH peer review system.
A proposed Clinical Trial application may include study design, methods, and intervention that are not by themselves innovative but address important questions or unmet needs. Additionally, the results of the clinical trial may indicate that further clinical development of the intervention is unwarranted or lead to new avenues of scientific investigation.
Overall Impact
Reviewers will provide an overall impact score to reflect their assessment of the likelihood for the project to exert a sustained, powerful influence on the research field(s) involved, in consideration of the following review criteria and additional review criteria (as applicable for the project proposed). As part of the overall impact score, reviewers should consider and indicate how the Plan to Enhance Diverse Perspectives affects the scientific merit of the project.
Scored Review Criteria
Reviewers will consider each of the review criteria below in the determination of scientific merit and give a separate score for each. An application does not need to be strong in all categories to be judged likely to have major scientific impact. For example, a project that by its nature is not innovative may be essential to advance a field.
Significance
Does the project address an important problem or a critical barrier to progress in the field? Is the prior research that serves as the key support for the proposed project rigorous? If the aims of the project are achieved, how will scientific knowledge, technical capability, and/or clinical practice be improved? How will successful completion of the aims change the concepts, methods, technologies, treatments, services, or preventative interventions that drive this field?
Are the scientific rationale and need for a clinical trial to test the proposed hypothesis or intervention well supported by preliminary data, clinical and/or preclinical studies, or information in the literature or knowledge of biological mechanisms? For trials focusing on clinical or public health endpoints, is this clinical trial necessary for testing the safety, efficacy or effectiveness of an intervention that could lead to a change in clinical practice, community behaviors or health care policy? For trials focusing on mechanistic, behavioral, physiological, biochemical, or other biomedical endpoints, is this trial needed to advance scientific understanding?
Specific to this NOFO:
- To what extent does the application address questions related to preventing opioid and/or stimulant-related morbidity and mortality for justice-involved populations?
- To what extent does the application address, generalizable treatment models in justice settings?
- To what extent does the application generate novel information about how to improve collaborations between justice and community-based/behavioral health providers to improve public health and public safety outcomes?
- To what extent does the research plan address potential sustainability and scalability?
Investigator(s)
Are the PD(s)/PI(s), collaborators, and other researchers well suited to the project? If Early Stage Investigators or those in the early stages of independent careers, do they have appropriate experience and training? If established, have they demonstrated an ongoing record of accomplishments that have advanced their field(s)? If the project is collaborative or multi-PD/PI, do the investigators have complementary and integrated expertise; are their leadership approach, governance, and organizational structure appropriate for the project?
With regard to the proposed leadership for the project, do the PD/PI(s) and key personnel have the expertise, experience, and ability to organize, manage and implement the proposed clinical trial and meet milestones and timelines? Do they have appropriate expertise in study coordination, data management and statistics? For a multicenter trial, is the organizational structure appropriate and does the application identify a core of potential center investigators and staffing for a coordinating center?
Specific to this NOFO:
- Is the time commitment of the PD/PI (s) and the investigators with decision-making authorities appropriate for the stated study goals?
- Is there clear description of roles for each major key personnel involved in the research site?
- Are senior leaders from relevant (a) justice settings AND (b) community-based or behavioral health service providers included, if applicable to the proposed project?
- If key personnel do not have a history of collaboration, is an appropriate plan in place to ensure successful coordination and communication?
Innovation
Does the application challenge and seek to shift current research or clinical practice paradigms by utilizing novel theoretical concepts, approaches or methodologies, instrumentation, or interventions? Are the concepts, approaches or methodologies, instrumentation, or interventions novel to one field of research or novel in a broad sense? Is a refinement, improvement, or new application of theoretical concepts, approaches or methodologies, instrumentation, or interventions proposed?
Does the design/research plan include innovative elements, as appropriate, that enhance its sensitivity, potential for information or potential to advance scientific knowledge or clinical practice?
Approach
Are the overall strategy, methodology, and analyses well-reasoned and appropriate to accomplish the specific aims of the project? Have the investigators included plans to address weaknesses in the rigor of prior research that serves as the key support for the proposed project? Have the investigators presented strategies to ensure a robust and unbiased approach, as appropriate for the work proposed? Are potential problems, alternative strategies, and benchmarks for success presented? If the project is in the early stages of development, will the strategy establish feasibility and will particularly risky aspects be managed? Have the investigators presented adequate plans to address relevant biological variables, such as sex, for studies in vertebrate animals or human subjects?
If the project involves human subjects and/or NIH-defined clinical research, are the plans to address 1) the protection of human subjects from research risks, and 2) inclusion (or exclusion) of individuals on the basis of sex/gender, race, and ethnicity, as well as the inclusion or exclusion of individuals of all ages (including children and older adults), justified in terms of the scientific goals and research strategy proposed?
Does the application adequately address the following, if applicable
Study Design
Is the study design justified and appropriate to address primary and secondary outcome variable(s)/endpoints that will be clear, informative and relevant to the hypothesis being tested? Is the scientific rationale/premise of the study based on previously well-designed preclinical and/or clinical research? Given the methods used to assign participants and deliver interventions, is the study design adequately powered to answer the research question(s), test the proposed hypothesis/hypotheses, and provide interpretable results? Is the trial appropriately designed to conduct the research efficiently? Are the study populations (size, gender, age, demographic group), proposed intervention arms/dose, and duration of the trial, appropriate and well justified?
Are potential ethical issues adequately addressed? Is the process for obtaining informed consent or assent appropriate? Is the eligible population available? Are the plans for recruitment outreach, enrollment, retention, handling dropouts, missed visits, and losses to follow-up appropriate to ensure robust data collection? Are the planned recruitment timelines feasible and is the plan to monitor accrual adequate? Has the need for randomization (or not), masking (if appropriate), controls, and inclusion/exclusion criteria been addressed? Are differences addressed, if applicable, in the intervention effect due to sex/gender and race/ethnicity?
Are the plans to standardize, assure quality of, and monitor adherence to, the trial protocol and data collection or distribution guidelines appropriate? Is there a plan to obtain required study agent(s)? Does the application propose to use existing available resources, as applicable?
Data Management and Statistical Analysis
Are planned analyses and statistical approach appropriate for the proposed study design and methods used to assign participants and deliver interventions? Are the procedures for data management and quality control of data adequate at clinical site(s) or at center laboratories, as applicable? Have the methods for standardization of procedures for data management to assess the effect of the intervention and quality control been addressed? Is there a plan to complete data analysis within the proposed period of the award?
Specific to this NOFO:
- Does the applicant propose an implementation or hybrid-implementation effectiveness research design?
- Does the Stakeholder Engagement and Dissemination Plan include a plan for engaging individuals with lived experience and stakeholders that is explicit with regard to engagement prior to study launch, during study execution, and plans for meaningful sharing of results with relevant stakeholders?
Environment
Will the scientific environment in which the work will be done contribute to the probability of success? Are the institutional support, equipment, and other physical resources available to the investigators adequate for the project proposed? Will the project benefit from unique features of the scientific environment, subject populations, or collaborative arrangements?
If proposed, are the administrative, data coordinating, enrollment and laboratory/testing centers, appropriate for the trial proposed?
Does the application adequately address the capability and ability to conduct the trial at the proposed site(s) or centers? Are the plans to add or drop enrollment centers, as needed, appropriate?
If international site(s) is/are proposed, does the application adequately address the complexity of executing the clinical trial?
If multi-sites/centers, is there evidence of the ability of the individual site or center to: (1) enroll the proposed numbers; (2) adhere to the protocol; (3) collect and transmit data in an accurate and timely fashion; and, (4) operate within the proposed organizational structure?
Additional Review Criteria
As applicable for the project proposed, reviewers will evaluate the following additional items while determining scientific and technical merit, and in providing an overall impact score, but will not give separate scores for these items.
Study Timeline
Is the study timeline described in detail, taking into account start-up activities, the anticipated rate of enrollment, and planned follow-up assessment? Is the projected timeline feasible and well justified? Does the project incorporate efficiencies and utilize existing resources (e.g., CTSAs, practice-based research networks, electronic medical records, administrative database, or patient registries) to increase the efficiency of participant enrollment and data collection, as appropriate?
Are potential challenges and corresponding solutions discussed (e.g., strategies that can be implemented in the event of enrollment shortfalls)?
Protections for Human Subjects
For research that involves human subjects but does not involve one of the categories of research that are exempt under 45 CFR Part 46, the committee will evaluate the justification for involvement of human subjects and the proposed protections from research risk relating to their participation according to the following five review criteria: 1) risk to subjects, 2) adequacy of protection against risks, 3) potential benefits to the subjects and others, 4) importance of the knowledge to be gained, and 5) data and safety monitoring for clinical trials.
For research that involves human subjects and meets the criteria for one or more of the categories of research that are exempt under 45 CFR Part 46, the committee will evaluate: 1) the justification for the exemption, 2) human subjects involvement and characteristics, and 3) sources of materials. For additional information on review of the Human Subjects section, please refer to the Guidelines for the Review of Human Subjects.
Inclusion of Women, Minorities, and Individuals Across the Lifespan
When the proposed project involves human subjects and/or NIH-defined clinical research, the committee will evaluate the proposed plans for the inclusion (or exclusion) of individuals on the basis of sex/gender, race, and ethnicity, as well as the inclusion (or exclusion) of individuals of all ages (including children and older adults) to determine if it is justified in terms of the scientific goals and research strategy proposed. For additional information on review of the Inclusion section, please refer to the Guidelines for the Review of Inclusion in Clinical Research.
Vertebrate Animals
The committee will evaluate the involvement of live vertebrate animals as part of the scientific assessment according to the following three points: (1) a complete description of all proposed procedures including the species, strains, ages, sex, and total numbers of animals to be used; (2) justifications that the species is appropriate for the proposed research and why the research goals cannot be accomplished using an alternative non-animal model; and (3) interventions including analgesia, anesthesia, sedation, palliative care, and humane endpoints that will be used to limit any unavoidable discomfort, distress, pain and injury in the conduct of scientifically valuable research. Methods of euthanasia and justification for selected methods, if NOT consistent with the AVMA Guidelines for the Euthanasia of Animals, is also required but is found in a separate section of the application. For additional information on review of the Vertebrate Animals Section, please refer to the Worksheet for Review of the Vertebrate Animals Section.
Biohazards
Reviewers will assess whether materials or procedures proposed are potentially hazardous to research personnel and/or the environment, and if needed, determine whether adequate protection is proposed.
Resubmissions
Not Applicable.
Renewals
Not Applicable.
Revisions
Not Applicable.
As applicable for the project proposed, reviewers will consider each of the following items, but will not give scores for these items, and should not consider them in providing an overall impact score.
Applications from Foreign Organizations
Not Applicable.
Select Agent Research
Reviewers will assess the information provided in this section of the application, including 1) the Select Agent(s) to be used in the proposed research, 2) the registration status of all entities where Select Agent(s) will be used, 3) the procedures that will be used to monitor possession use and transfer of Select Agent(s), and 4) plans for appropriate biosafety, biocontainment, and security of the Select Agent(s).
Resource Sharing Plans
Reviewers will comment on whether the Resource Sharing Plan(s) (i.e., Sharing Model Organisms) or the rationale for not sharing the resources, is reasonable.
Authentication of Key Biological and/or Chemical Resources:
For projects involving key biological and/or chemical resources, reviewers will comment on the brief plans proposed for identifying and ensuring the validity of those resources.
Budget and Period of Support
Reviewers will consider whether the budget and the requested period of support are fully justified and reasonable in relation to the proposed research.
2. Review and Selection Process
Applications will be evaluated for scientific and technical merit by (an) appropriate Scientific Review Group(s) convened by NIDA, in accordance with NIH peer review policy and procedures, using the stated review criteria. Assignment to a Scientific Review Group will be shown in the eRA Commons.
As part of the scientific peer review, all applications will receive a written critique.
Applications may undergo a selection process in which only those applications deemed to have the highest scientific and technical merit (generally the top half of applications under review) will be discussed and assigned an overall impact score.
Appeals of initial peer review will not be accepted for applications submitted in response to this NOFO.
Applications will be assigned to the appropriate NIH Institute or Center. Applications will compete for available funds with all other recommended applications submitted in response to this NOFO. Following initial peer review, recommended applications will receive a second level of review by the National Advisory Council on Drug Abuse.
The following will be considered in making funding decisions:
- Scientific and technical merit of the proposed project, including the PEDP, as determined by scientific peer review.
- Availability of funds.
- Relevance of the proposed project to program priorities.
3. Anticipated Announcement and Award Dates
After the peer review of the application is completed, the PD/PI will be able to access his or her Summary Statement (written critique) via the eRA Commons. Refer to Part 1 for dates for peer review, advisory council review, and earliest start date.
Information regarding the disposition of applications is available in the NIH Grants Policy Statement Section 2.4.4 Disposition of Applications.
1. Award Notices
If the application is under consideration for funding, NIH will request "just-in-time" information from the applicant as described in the NIH Grants Policy Statement. This request is not a Notice of Award nor should it be construed to be an indicator of possible funding.
A formal notification in the form of a Notice of Award (NoA) will be provided to the applicant organization for successful applications. The NoA signed by the grants management officer is the authorizing document and will be sent via email to the recipient's business official.
Recipients must comply with any funding restrictions described in Section IV.6. Funding Restrictions. Selection of an application for award is not an authorization to begin performance. Any costs incurred before receipt of the NoA are at the recipient's risk. These costs may be reimbursed only to the extent considered allowable pre-award costs.
Any application awarded in response to this NOFO will be subject to terms and conditions found on the Award Conditions and Information for NIH Grants website. This includes any recent legislation and policy applicable to awards that is highlighted on this website.
Individual awards are based on the application submitted to, and as approved by, the NIH and are subject to the IC-specific terms and conditions identified in the NoA.
ClinicalTrials.gov: If an award provides for one or more clinical trials. By law (Title VIII, Section 801 of Public Law 110-85), the "responsible party" must register and submit results information for certain “applicable clinical trials” on the ClinicalTrials.gov Protocol Registration and Results System Information Website (https://register.clinicaltrials.gov). NIH expects registration and results reporting of all trials whether required under the law or not. For more information, see https://grants.nih.gov/policy/clinical-trials/reporting/index.htm
Institutional Review Board or Independent Ethics Committee Approval: Recipient institutions must ensure that all protocols are reviewed by their IRB or IEC. To help ensure the safety of participants enrolled in NIH-funded studies, the recipient must provide NIH copies of documents related to all major changes in the status of ongoing protocols.
Data and Safety Monitoring Requirements: The NIH policy for data and safety monitoring requires oversight and monitoring of all NIH-conducted or -supported human biomedical and behavioral intervention studies (clinical trials) to ensure the safety of participants and the validity and integrity of the data. Further information concerning these requirements is found at http://grants.nih.gov/grants/policy/hs/data_safety.htm and in the application instructions (SF424 (R&R) and PHS 398).
Investigational New Drug or Investigational Device Exemption Requirements: Consistent with federal regulations, clinical research projects involving the use of investigational therapeutics, vaccines, or other medical interventions (including licensed products and devices for a purpose other than that for which they were licensed) in humans under a research protocol must be performed under a Food and Drug Administration (FDA) investigational new drug (IND) or investigational device exemption (IDE).
2. Administrative and National Policy Requirements
All NIH grant and cooperative agreement awards include the NIH Grants Policy Statement as part of the NoA. For these terms of award, see the NIH Grants Policy Statement Part II: Terms and Conditions of NIH Grant Awards, Subpart A: General and Part II: Terms and Conditions of NIH Grant Awards, Subpart B: Terms and Conditions for Specific Types of Grants, Recipients, and Activities, including of note, but not limited to:
- Federal-wide Standard Terms and Conditions for Research Grants
- Prohibition on Certain Telecommunications and Video Surveillance Services or Equipment
- Acknowledgment of Federal Funding
If a recipient is successful and receives a Notice of Award, in accepting the award, the recipient agrees that any activities under the award are subject to all provisions currently in effect or implemented during the period of the award, other Department regulations and policies in effect at the time of the award, and applicable statutory provisions.
If a recipient receives an award, the recipient must follow all applicable nondiscrimination laws. The recipient agrees to this when registering in SAM.gov. The recipient must also submit an Assurance of Compliance (HHS-690). To learn more, see the Laws and Regulations Enforced by the HHS Office for Civil Rights website.
HHS recognizes that NIH research projects are often limited in scope for many reasons that are nondiscriminatory, such as the principal investigator’s scientific interest, funding limitations, recruitment requirements, and other considerations. Thus, criteria in research protocols that target or exclude certain populations are warranted where nondiscriminatory justifications establish that such criteria are appropriate with respect to the health or safety of the subjects, the scientific study design, or the purpose of the research. For additional guidance regarding how the provisions apply to NIH grant programs, please contact the Scientific/Research Contact that is identified in Section VII under Agency Contacts of this NOFO.
In accordance with the statutory provisions contained in Section 872 of the Duncan Hunter National Defense Authorization Act of Fiscal Year 2009 (Public Law 110-417), NIH awards will be subject to System for Award Management (SAM.gov) requirements. SAM.gov requires Federal agencies to review and consider information about an applicant in the designated integrity and performance system (currently SAM.gov) prior to making an award. An applicant can review and comment on any information in the responsibility/qualification records available in SAM.gov. NIH will consider any comments by the applicant, in addition to the information available in the responsibility/qualification records in SAM.gov, in making a judgement about the applicant’s integrity, business ethics, and record of performance under Federal awards when completing the review of risk posed by applicants as described in 2 CFR Part 200.206 “Federal awarding agency review of risk posed by applicants.” This provision will apply to all NIH grants and cooperative agreements except fellowships.
The following special terms of award are in addition to, and not in lieu of, otherwise applicable U.S. Office of Management and Budget (OMB) administrative guidelines, U.S. Department of Health and Human Services (HHS) grant administration regulations at 2 CFR Part 200, and other HHS, PHS, and NIH grant administration policies.
The administrative and funding instrument used for this program will be the cooperative agreement, an "assistance" mechanism (rather than an "acquisition" mechanism), in which substantial NIH programmatic involvement with the recipients is anticipated during the performance of the activities. Under the cooperative agreement, the NIH purpose is to support and stimulate the recipients' activities by involvement in and otherwise working jointly with the recipients in a partnership role; it is not to assume direction, prime responsibility, or a dominant role in the activities. Consistent with this concept, the dominant role and prime responsibility resides with the recipients for the project as a whole, although specific tasks and activities may be shared among the recipients and NIH as defined below.
The PD(s)/PI(s) will have the primary responsibility for:
- Organizing a local Executive Committee for day-to-day management of the study.
- Ensuring cooperation and coordination with the CTC, the MAARC, the ERRC, and the CERRC. This includes ensuring data uploads are provided in a timely fashion to the MAARC.
- Serving as a member of the JCOIN SC and participating in required activities, including primary responsibility for hosting annual virtual site visits.
- Participating in the overall coordination of NIH research efforts in justice settings. This participation may include collaboration and consultation with other NIH recipients, the appropriate sharing of information, data, and research materials, and participation in NIH efforts to standardize and harmonize pre-clinical and clinical data collection.
- Provide updates at least annually on progress in PEDP implementation.
Recipients will retain custody of and have primary rights to the data and software developed under these awards, subject to Government rights of access consistent with current HHS, PHS, and NIH policies.
NIH staff have substantial programmatic involvement that is above and beyond the normal stewardship role in awards, as described below:
- The NIH Project Scientist(s) will work closely with the PD(s)/PI(s), the SC, and the PIs of all JCOIN network components in order to ensure proper conduct of all network activities.
- The NIH Project Scientist(s) will have one (1) vote on the SC, regardless of how many NIH Project Scientists participate across the network.
- The assigned Project Scientist(s) will be responsible for: (1) providing advice and guidance to the Clinical Research Hub to ensure that their studies are consistent with the goals of JCOIN and are of high scientific priority and utility; (2) serving as a point of contact for investigators with the NIH; (3) coordinating and approving collaborative projects between the Hub and other recipients; and (4) connecting and coordinating among all components of the JCOIN network to ensure overall success of the network and operation as a collaborative endeavor.
- Additionally, an agency program official or IC program director will be responsible for the normal scientific and programmatic stewardship of the award and will be named in the award notice.
- NIDA, as the primary funder and administrator, reserves the right to phase out or curtail the award (or an individual component of the award) in the event of inadequate progress or data reporting. NIH support of this study is contingent upon adequate study progress based on the Grantee’s Milestone Plan submitted at the time of funding.
Areas of Joint Responsibility include:
- The SC is the primary governing body of the Cooperative. Recipients must participate in the SC. The SC or its designated committees develops and monitors policies and procedures guiding the network, and serves as a forum to facilitate collaboration, identify research gaps and opportunities, and integrate insights from practitioners. Recipients agree to abide by the procedures and policies established by the SC.
- Data Management, Analysis, and Access: Data generated are the property of the awardee. Research sites must provide requested data to the CTC, MAARC, ERRC, and CERRC (as appropriate) in a timely fashion in accordance with the policies and procedures established in study protocols and by the SC. In addition, the CTC, MAARC, EERC, and CERRC and all research sites must provide NIDA with access to all data generated under this award, subject to rules specified in any Certificates of Confidentiality obtained by recipients. Data must be shared upon request with the SC and subcommittees reporting to the SC when appropriate.
- JCOIN is intended to be a national resource, and as such, each Clinical Research Center must be prepared to share their data under provisions that safeguard the privacy and confidentiality of respondents.
- Recipients and NIDA will jointly develop appropriate confidentiality procedures for data collection, processing, storage and analysis to ensure the confidentiality of data.
- All recipients and NIDA will cooperate to ensure the timely and broad dissemination of lessons learned, to inform researchers and health care systems engaged in research and beyond.
- The SC, with the support of the CTC, will facilitate these joint activities and, in particular, development of research protocols, human subjects and other regulatory protocols, data harmonization, manuscript and other information dissemination planning, and initial clearance of manuscripts or other dissemination products.
Dispute Resolution:
Any disagreements that may arise in scientific or programmatic matters (within the scope of the award) between recipients and NIH may be brought to Dispute Resolution. A Dispute Resolution Panel composed of three members will be convened: a designee of the SC chosen without NIH staff voting, one NIH designee, and a third designee with expertise in the relevant area who is chosen by the other two; in the case of individual disagreement, the first member may be chosen by the individual recipient. This special dispute resolution procedure does not alter the recipient's right to appeal an adverse action that is otherwise appealable in accordance with PHS regulation 42 CFR Part 50, Subpart D and HHS regulation 45 CFR Part 16.
3. Data Management and Sharing
Consistent with the 2023 NIH Policy for Data Management and Sharing, when data management and sharing is applicable to the award, recipients will be required to adhere to the Data Management and Sharing requirements as outlined in the NIH Grants Policy Statement. Upon the approval of a Data Management and Sharing Plan, it is required for recipients to implement the plan as described.
HEAL Data Sharing Requirements
NIH intends to maximize the impact of HEAL Initiative-supported projects through broad and rapid data sharing. All HEAL Initiative award recipients, regardless of the amount of direct costs requested for any one year, are required to comply with the HEAL Public Access and Data Sharing Policy. HEAL award recipients must following all requirements and timelines developed through the HEAL Initiative Data Ecosystem (https://heal.nih.gov/about/heal-data-ecosystem), as described in HEAL’s compliance guidance (See Already Funded section: https://heal.nih.gov/data/complying-heal-data-sharing-policy):
1. Select a HEAL Compliant data repository (https://www.healdatafair.org/resources/guidance/selection)
- Data generated by HEAL Initiative-funded projects must be submitted to study-appropriate, HEAL-compliant, data repositories to ensure the data is accessible via the HEAL Initiative Data Ecosystem.
- Some repositories require use of specific data dictionaries or structured data elements, so knowing your repository’s requirements up front can help reduce the burden of preparing data for submission.
- HEAL-funded recipients must follow requirements for selected repository
2. Within one year of award, register your study with the HEAL platform (https://heal.github.io/platform-documentation/study-registration/)
- This process will connect the Platform to information about your study and data, including metadata, and identify the selected repository. HEAL requests initial submission within one year of award, with annual updates, and to be updated in accordance with any release of study data.
3. Within one year of award, submit HEAL-specific study-level metadata.
- Some of the required study-level metadata (https://github.com/HEAL/heal-metadata-schemas/blob/main/for-investigators-how-to/study-level-metadata-fields/study-metadata-schema-for-humans.pdf) will be auto-populated as part of the registration process.
4. Submit data and metadata (and code, if applicable) to HEAL-Compliant repository
- At the completion of the study and/or when prepared to make the final data deposits in the repositor(ies) of choice, ensure your study registration (https://heal.github.io/platform-documentation/study-registration/) is complete.
- The NIH HEAL Initiative expects data used in publications to be submitted to repositories at the time of or prior to publication, and no later than the end of the project period.
5. Additional Requirements for HEAL Initiative studies conducting clinical research or research involving human subjects.
These studies must meet the following additional requirements:
- HEAL Initiative trials that are required to register in clinicaltrials.gov should reference support from and inclusion in the HEAL Initiative by including the standardized terms the HEAL Initiative (https://heal.nih.gov/) in the Study Description Section.
- All new HEAL clinical pain studies are required to use core questionnaires required by the HEAL Clinical Data Elements (CDE) Program (https://heal.nih.gov/data/common-data-elements). Outside of the core questionnaires, studies should select questionnaires from among the repository of supplemental questionnaires that are already being used by other HEAL clinical pain studies. The program has created the CDE files containing standardized variable names, responses, coding, and other information for all of these questionnaires The program has also formatted the case-report forms in a standardized way that is compliant with accessibility standards under Section 508 of the Rehabilitation Act of 1973 (29 U.S.C 794 (d); https://www.govinfo.gov/content/pkg/USCODE-2011-title29/html/USCODE-2011-title29-chap16-subchapV-sec794d.htm) which require[s] Federal agencies to make their electronic and information technology accessible to people with disabilities.
- Studies that wish to use questionnaires not already included in the HEAL CDE repository should consult with their program official and the HEAL CDE team. New questionnaires will be considered for inclusion in the repository on a case-by-case basis and only when appropriate justification is provided.
- HEAL Initiative clinical studies that are using copyrighted questionaries are required to obtain licenses for use prior to initiating data collection. Licenses must be shared with the HEAL CDE team and the program officer prior to use of copyrighted materials. For additional information, visit the HEAL CDE Program (https://heal.nih.gov/data/common-data-elements).
- To the extent possible, all other (non-pain) HEAL studies conducting clinical trials or research involving human subject are expected to use questionnaires by the HEAL Clinical Data Elements (CDE) Program (https://heal.nih.gov/data/common-data-elements) if applicable and relevant to their research.
- To the extent possible, HEAL recipients are expected to integrate broad data sharing consent language into their informed consent forms.
Additional details, resources, and tools to assist with data related activities can be found at https://www.healdatafair.org/.
All data collected as part of the NIH HEAL Initiative are so collected under a Certificate of Confidentiality and entitled to the protections thereof. Institutions who receive Data and/or Materials from this award for performance of activities under this award are required to use the Data and/or Materials only as outlined by the NIH HEAL Initiative, in a manner that is consistent with applicable state and federal laws and regulations, including any informed consent requirements and the terms of the institution’s NIH funding, including NOT-OD-17-109 and 42 U.S.C. 241(d). Failure to adhere to this criterion may result in enforcement actions.
4. Reporting
When multiple years are involved, recipients will be required to submit the Research Performance Progress Report (RPPR) annually and financial statements as required in the NIH Grants Policy Statement.
- Recipients will provide updates at least annually on implementation of the PEDP
Report and ensure immediate public access to HEAL-funded publications
Publications resulting from NIH HEAL Initiative funded studies must be immediately publicly available upon publication.
- For manuscripts published in journals that are not immediately open access, authors should arrange with journals in advance to pay for immediate open access
- Costs to ensure manuscripts are immediately publicly available upon publication should be included in budget requests
Prior to publication, HEAL expects investigators to alert their program officers of upcoming manuscripts to ensure coordination of communication and outreach efforts.
Award recipients and their collaborators are required to acknowledge HEAL Initiative support by referencing in the acknowledgment sections of any relevant publication:
“This research was supported by the National Institutes of Health through the NIH HEAL Initiative (https://heal.nih.gov) under award number [include specific grant/contract/award number; with NIH grant number(s) in this format: R01GM987654].”
A final RPPR, invention statement, and the expenditure data portion of the Federal Financial Report are required for closeout of an award, as described in the NIH Grants Policy Statement. NIH NOFOs outline intended research goals and objectives. Post award, NIH will review and measure performance based on the details and outcomes that are shared within the RPPR, as described at 2 CFR Part 200.301.
The Federal Funding Accountability and Transparency Act of 2006 as amended (FFATA), includes a requirement for recipients of Federal grants to report information about first-tier subawards and executive compensation under Federal assistance awards issued in FY2011 or later. All recipients of applicable NIH grants and cooperative agreements are required to report to the Federal Subaward Reporting System (FSRS) available at www.fsrs.gov on all subawards over $25,000. See the NIH Grants Policy Statement for additional information on this reporting requirement.
In accordance with the regulatory requirements provided at 2 CFR Part 200.113 and Appendix XII to 2 CFR Part 200, recipients that have currently active Federal grants, cooperative agreements, and procurement contracts from all Federal awarding agencies with a cumulative total value greater than $10,000,000 for any period of time during the period of performance of a Federal award, must report and maintain the currency of information reported in the System for Award Management (SAM) about civil, criminal, and administrative proceedings in connection with the award or performance of a Federal award that reached final disposition within the most recent five-year period. The recipient must also make semiannual disclosures regarding such proceedings. Proceedings information will be made publicly available in the designated integrity and performance system (Responsibility/Qualification in SAM.gov, formerly FAPIIS). This is a statutory requirement under section 872 of Public Law 110-417, as amended (41 U.S.C. 2313). As required by section 3010 of Public Law 111-212, all information posted in the designated integrity and performance system on or after April 15, 2011, except past performance reviews required for Federal procurement contracts, will be publicly available. Full reporting requirements and procedures are found in Appendix XII to 2 CFR Part 200 – Award Term and Conditions for Recipient Integrity and Performance Matters.
We encourage inquiries concerning this funding opportunity and welcome the opportunity to answer questions from potential applicants.
eRA Service Desk (Questions regarding ASSIST, eRA Commons, application errors and warnings, documenting system problems that threaten submission by the due date, and post-submission issues)
Finding Help Online: https://www.era.nih.gov/need-help (preferred method of contact)
Telephone: 301-402-7469 or 866-504-9552 (Toll Free)
General Grants Information (Questions regarding application instructions, application processes, and NIH grant resources)
Email: [email protected] (preferred method of contact)
Telephone: 301-637-3015
Grants.gov Customer Support (Questions regarding Grants.gov registration and Workspace)
Contact Center Telephone: 800-518-4726
Email: [email protected]
Carrie Mulford, PhD
National Institute on Drug Abuse (NIDA)
Phone: 301-827-6473
Email: [email protected]
Denise L Stredrick, PhD
Office of Disease Prevention (ODP)
Phone: 301-594-7553
E-mail: [email protected]
Dharmendar Rathore, PhD
National Institute on Drug Abuse (NIDA)
Phone: 301-402-6965
Email: [email protected]
Ericka Wells
National Institute on Drug Abuse (NIDA)
Phone: 301-827-6705
Email: [email protected]
Recently issued trans-NIH policy notices may affect your application submission. A full list of policy notices published by NIH is provided in the NIH Guide for Grants and Contracts. All awards are subject to the terms and conditions, cost principles, and other considerations described in the NIH Grants Policy Statement.
Awards are made under the authorization of Sections 301 and 405 of the Public Health Service Act as amended (42 USC 241 and 284) and under Federal Regulations 42 CFR Part 52 and 2 CFR Part 200.
and Human Services (HHS)