National Institutes of Health (NIH)
See Notices of Special Interest associated with this funding opportunity
NOT-OD-22-190 - Adjustments to NIH and AHRQ Grant Application Due Dates Between September 22 and September 30, 2022
September 28, 2022 - Notice of Pre-Application Technical Assistance Webinar for NIDA RFA-DA-23-057 and RFA-DA-23-058. See Notice NOT-DA-22-080.
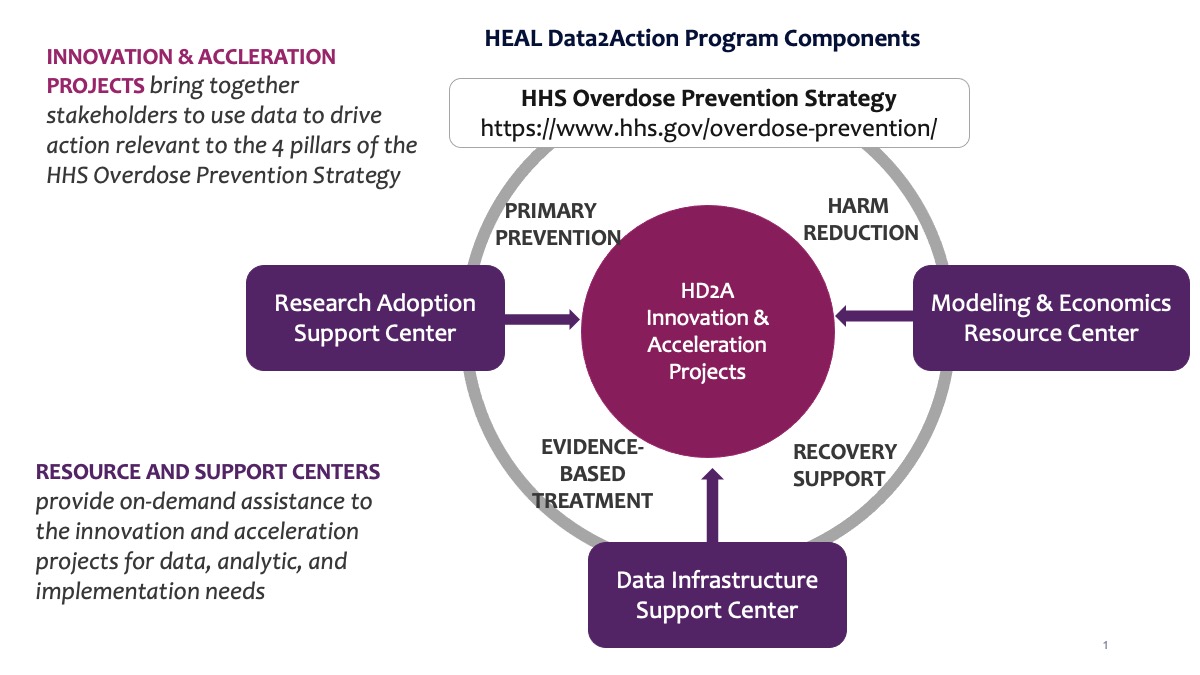
As part of the NIH HEAL Initiative, the National Institute on Drug Abuse (NIDA) is releasing a set of interrelated Funding Opportunity Announcements (FOAs) to create the HEAL Data2Action (HD2A) Program, a coordinated effort to promote the synthesis and real-world application of existing data to improve epidemiology and guide and monitor improvements in service delivery to prevent or treat opioid use disorder (OUD) and pain. Collectively, these projects will improve the quality, timeliness, accessibility and usefulness of data for epidemiology and service delivery in each of the four pillars of the HHS Overdose Prevention Strategy: primary prevention, harm reduction, treatment of opioid use disorder, and recovery support. Separate FOAs have been issued to support multiple HD2A Innovation Projects (RFA-DA-22-051); one HD2A Data Infrastructure Support Center (RFA-DA-22-052); one HD2A Research Adoption Support Center (RFA-DA-22-050); and one HD2A Economics and Modeling Resource Center (RFA-DA-22-049). It is imperative that prospective applicants read all of these related RFAs to better understand the intended purpose and structure of the HD2A Program.
This FOA seeks applications for HEAL Data2Action (HD2A) Projects. Research Projects will focus on one of two priorities: Priority 1 develop data or methods that improves the timeliness, quality, accessibility or usefulness of existing data ecosystems (Acceleration Projects) or Priority 2 - leveraging single system or cross-sector partnerships to use data to identify and fill service delivery gaps with evidence-based strategies and monitor improvements (Innovation Projects). Applicants should specify which Priority they are responding to in their applications. This FOA invites phased applications to support projects for which preliminary or feasibility data are not available at the time of submission. This FOA is a companion to RFA-DA-23-058, which seeks applications for Acceleration Projects for which pilot data are available. It is expected that the Data Infrastructure Support Center (RFA-DA-22-052), the Modeling and Economic Resource Center (RFA-DA-22-049), and the Research Adoption Support Center (RFA-DA-22-050) will support projects funded under this announcement. All projects funded under this announcement will allow for faster and improved responses and allocation of resources, as well as deployment of evidence-based practices to address the overdose crisis.
October 22, 2022
| Application Due Dates | Review and Award Cycles | ||||
|---|---|---|---|---|---|
| New | Renewal / Resubmission / Revision (as allowed) | AIDS | Scientific Merit Review | Advisory Council Review | Earliest Start Date |
| November 22, 2022 | November 22, 2022 | Not Applicable | March 2023 | May 2023 | July 2023 |
All applications are due by 5:00 PM local time of applicant organization.
Applicants are encouraged to apply early to allow adequate time to make any corrections to errors found in the application during the submission process by the due date.
Not Applicable
It is critical that applicants follow the instructions in the Research (R) Instructions in the SF424 (R&R) Application Guide, except where instructed to do otherwise (in this FOA or in a Notice from NIH Guide for Grants and Contracts).
Conformance to all requirements (both in the Application Guide and the FOA) is required and strictly enforced. Applicants must read and follow all application instructions in the Application Guide as well as any program-specific instructions noted in Section IV. When the program-specific instructions deviate from those in the Application Guide, follow the program-specific instructions.
Applications that do not comply with these instructions may be delayed or not accepted for review.
Background: HEAL Initiative
This study is part of the NIH’s Helping to End Addiction Long-term (HEAL) initiative to speed scientific solutions to the national opioid public health crisis. The NIH HEAL Initiative bolsters research across NIH to (1) improve treatment for opioid misuse and addiction and (2) enhance pain management. More information about the HEAL Initiative is available at: https://heal.nih.gov/.
Background: HEAL Data2Action (HD2A) Program
In the 12-month period ending in December 2021, more than 100,000 people lost their lives to overdose deaths. Deaths have continued to rise despite significant efforts and resources aimed at reversing these trends. Challenges related to rapidly collecting, interpreting, and using high-quality data to drive decisions and deploy resources in real time represents a major barrier to reversing these trends. At the same time, reductions in opioid prescribing have raised challenges for adults in the U.S. struggling with chronic pain, with a need to ensure that comprehensive, evidence-based pain management approaches are utilized. The HEAL Data2Action (HD2A) Program is intended to promote near real-time use of available data by health systems, communities, and related stakeholders to improve epidemiology, forecast service delivery needs, identify gaps, and inform proactive responses in line with the 4 key pillars of the HHS Overdose Prevention Strategy: primary prevention (including effective pain management, appropriate opioid prescribing), harm reduction, treatment of opioid use disorder, and recovery support. HD2A Projects will work independently to identify, merge, and analyze data to address data and service gaps along the overdose prevention and opioid care cascade. Three support centers will provide technical assistance and related resources to assist the HD2A Projects in achieving their goals. Applicants to this FOA are strongly encouraged to review the FOAs for HD2A Data Infrastructure Support Center (RFA-DA-22-052), the HD2A Research Adoption Support Center (RFA-DA-22-050), and the HD2A Modeling and Economic Resource Center (RFA-DA-22-049) to understand the scope and structure of the HD2A Program.
A visual depiction of the structure and organization of this initiative can be found here: https://www.drugabuse.gov/sites/default/files/data_to_action.jpg.
{kind=link}
HEAL Data2Action (HD2A) Projects: Purpose and Scope of Activities
HEAL Data to Action (HD2A) Projects are phased awards intended to address one of two priorities:
- Priority 1 Acceleration Projects: develop data or methods that improve timeliness, quality, accessibility, or usefulness of existing data ecosystems (e.g., electronic health records, syndromic surveillance systems, claims data, registries, pharmacy dispensing, mortality records) to allow faster and improved responses to address the overdose epidemic.
- Priority 2 Innovation Projects: Leverage single system or cross-sector partnerships to use data to identify and fill service delivery gaps with evidence-based strategies and monitor improvements.
Applicants should specify which Priority they are responding to in their applications.
Priority 1: Acceleration Projects
Acceleration Projects are to develop data or methods that improve the timeliness, quality, accessibility, or usefulness of existing data ecosystems (e.g., electronic health records, syndromic surveillance, claims data, registry data, pharmacy dispensing, and mortality records) to allow for faster and improved responses to address the overdose epidemic.
The data or methods must focus on outcomes of interest to the HEAL initiative (e.g., opioid use disorder (OUD), overdose, relapse, chronic pain) or the HHS overdose prevention strategy. Priority will be given to applications that demonstrate the following: 1) translatability of the data or methods to other substance use problems, 2) identification and partnerships with stakeholders/end-users along the research continuum and inclusion of at least one representative of those end-users as a key personnel in the application to ensure that the proposed data or methods will be useful to the stakeholders who drive actions, and 3) evaluation and/or implementation of data or methods in terms of timeliness, quality, accessibility, or usefulness of data for prevention and services planning. There is no requirement or expectation that the data or methods will be used to drive action as part of the award activities.
Applications should describe how the data or methods proposed could be applicable to solving current problems. This may include facilitating the extraction and transformation of data from electronic health records (EHR) for research use and consideration of social determinants of health as crucial contributors to health. This is an opportunity to foster the adoption of standardized data structure such as Fast Healthcare interoperability Resources (FHIR ) in accessing and exchanging data from EHR.
The datasets produced, when applicable, shall adhere to the FAIR principles (Findable, Accessible, Interoperable, Reproducible) and shall be ethically sourced, trustworthy, well-defined, and accessible. The principles also apply to algorithms and other digital assets. The end products of this effort are twofold: 1) methods, algorithms, tools, or technologies that shorten the time lag between data capture and data availability or improve the geographical precision of available data, and 2) linked/integrated datasets or datasets that can be further integrated in an established data ecosystem that improves timeliness, quality, accessibility, or usefulness of the data to provide actionable insights.
Applications are phased awards. Support will be provided for a maximum of 5 years combining the R61 and R33 phases, which includes initial support of up to 2 years under an R61 phase, followed by up to 4 years of support for the R33 phase upon successfully meeting R61 milestones (i.e., phased award). Under the R61 phase, applicants will assess data system infrastructure needs and limitations, engage stakeholders, and identify methods for data improvement to meet potential use case needs.
Under the R33 award, applicants will develop data or methods and in terms of data timeliness, quality, accessibility, or usefulness that could apply to at least one use case (e.g., improvements in monitoring, early detection, hot spot identification, linkage and modeling for data-driven decision making).
The HD2A Program includes Support Centers that will provide technical assistance and other support to participating HD2A Projects. For Acceleration Projects, the resource centers are intended to assist Projects, for example, in informing benefits and tradeoffs of different data tools, applying simulation modeling in support of forecasting and decision-making, and understanding evidence-based practices that could serve as use cases. Each Acceleration Project will be expected to participate in a baseline needs assessment meeting with the Support Centers to identify opportunities and options for their proposed projects. Acceleration Projects will have an opportunity to access ongoing and on-demand support from each of these resource centers, as relevant and appropriate, throughout the course of the project.
Based on data and input from relevant stakeholders and considering the support available from the HD2A Support Centers, applicants should propose projects likely to have a measurable and sustained impact on overdose, opioid-related outcomes, and/or chronic pain, as relevant to their targeted element(s) of the Overdose Prevention Strategy, i.e., primary prevention, harm reduction, treatment of opioid use disorder, and recovery support.
Some examples of projects considered responsive to the Acceleration priority include but are not limited to the following:
- Enhance or develop methods for forecasting or nowcasting small-area or local estimates to inform public health officials where to allocate public health resources or develop data visualization and dissemination tools for small area estimation or local estimates (e.g., including a feature to implement outbreak detection or spatial outlier detection methods to identify counties or small areas)
- Improve prediction or assessment tools to identify individuals at increased risk for developing substance use disorders using near real-time or real-time data (e.g., social media, EHR)
- Enhance methods to identify and include individuals who misuse opioid or have OUD who are outside the formal medical treatment system (e.g., syringe service programs (SSPs) data) in the existing data ecosystem
- Enhance quality, timeliness, and usefulness of data to monitor the use, safety, and effectiveness of prescription opioids in acute or chronic pain management in the context of other evidence-based pain management strategies, and assess the benefits and risks of long-term opioid prescribing for chronic pain
- Develop methods that can efficiently link data from diverse systems for trackable datasets aggregation or evaluate optimal linkage of data from multiple sources (e.g., incorporation of the drug market data with near or real-time data to understand emerging drug problems) and generate data sources or public health data warehouse that can assemble a bigger picture for opioids misuse to address fundamental issues in prevention, treatment, management, and harm reduction
- Develop methods to capture data on illicit opioid usage on a near or real-time basis
- Enhance existing tools, algorithms, or methodologies through additional data, automation, or increased interoperability (e.g., methods to track and categorize emerging illicit drugs, increasing interoperability and automation for data from laboratories and medical examiner/coroner’s office to increase the timeliness of incorporating the information in an existing surveillance system, improve technologies or algorithms to mine or automatically extract unstructured data)
- Explore methods to model the contribution of illicit opioid drug use on other causes of death, especially for deaths not explicitly recorded as drug overdose or drug-related
Relevant data sets may include but are not limited to:
- Data collected through unique tools, methodologies, technologies, or other innovative means (e.g., datasets from mobile devices captured, social media data, web-based data)
- Data collected through local, state, or tribal government agencies (e.g., State birth and death registry, existing nationally representative data, syndromic surveillance data, residential or community service facility data)
- NIH-supported datasets that are being generated under investigator-initiated research (applicants should describe how they will access data, e.g., through existing repositories or working with collaborators)
- Data collected through nongovernment organizations such as administrative data from healthcare, clinic, and criminal justice settings (e.g., insurance claims, EHR, prescriptions, laboratory)
- Data from first responders or other sources integrated into local communities
Priority 2: Innovation Projects
Innovation Projects will use data to drive action and change in real-world settings with a Single System or Cross Sector partnership. The focus may include, but is not limited to, resource allocation; service delivery structure, staffing patterns; policy, practice or procedure changes; improving referrals and service linkages; adoption/implementation of evidence-based practices or measurement-based care; improving service quality, etc.
In the Single System Track, applications may identify key data-related gaps or inefficiencies that exist within a single, targeted system and propose an approach to improve use of existing data to identify service gaps and enhance service delivery. An example of a Single System application might involve a healthcare system that seeks to use data from one or multiple distinct service lines that operate under the same organizational structure.
In the Cross-Sector Track, applications may identify key data-related gaps or inefficiencies that require cross-sector partnerships to identify service gaps and improve service delivery. An example of a Cross-Sector project might involve a healthcare system partnering with community-based treatment providers and first responders to improve the transition of patients between emergency, primary, and specialty care. To maximize feasibility and ensure that the focus is on using data to inform action (rather than simply developing better methods of data integration), applicants are encouraged to limit the number of partnerships and justify the partnerships that will be established and including plans for how data will be integrated.
Across both tracks, examples of systems or stakeholders that could be engaged include, but are not limited to health systems, public health departments, behavioral health agencies, emergency departments, justice agencies, pain clinics, primary care clinics, Federally Qualified Health Centers, patient-advocacy groups, harm reduction agencies, recovery organizations, child welfare agencies, payers, and policy makers at local and state levels.
Innovation Projects in both tracks will be phased awards. Support will be provided for a maximum of 5 years combining the R61 and R33 phases, which includes initial support of up to 2 years of the R61 phase, followed by up to 4 years of support for the R33 phase upon successfully meeting R61 milestones, as described herein.
Across both tracks, Innovation Project efforts should focus on improving relevant aspects of the data infrastructure (e.g., data capture, data timeliness, data sharing, data linkage, data utilization etc.) as necessary to support data-driven decision-making and real-time feedback loops. The ultimate goal of proposed projects should be focused on using data to drive action and improve overdose-relevant outcomes, using a public health framework. Specifically, outcomes of the targeted actions must be relevant to at least one of the four key pillars of the HHS Overdose Prevention Strategy (primary prevention, harm reduction, treatment of opioid use disorder, and recovery support), and ideally project goals should be able to demonstrate near-term impacts. Applicants are strongly encouraged to directly address how, if successful, the targeted actions would have an impact on overdose and/or opioid-related morbidity and mortality outcomes. Alternatively, applicants could present a logic model for how, if successful, the proposed efforts are relevant to overdose and/or opioid-related morbidity and mortality and would have a meaningful impact on a related outcome. Applicants are strongly encouraged to implement systems and community-level strategies and assess outcomes at the broader community and systems levels, assessing impact beyond the individual level. Applications are also strongly encouraged to consider the relevance of the cascade of care (i.e., prevention, identification, referral, engagement and retention in care, and recovery support) as an organizing framework. Applications are further strongly encouraged to take issues of equity into consideration.
The HD2A Program includes three (3) Support Centers that will provide technical assistance and other support to participating Innovation Projects. These resource centers are intended to assist Innovation Projects in several ways, including: improving the utility of local data; applying simulation modeling in support of forecasting and decision-making; informing the selection of evidence-based practices and implementation strategies; and estimating the costs associated with various options and outcomes. Each Innovation Project will be expected to participate in a baseline needs assessment meeting with these centers to identify opportunities and options for their proposed projects. Innovation Projects will have access to ongoing and on-demand support from each of these resource centers throughout both phases of the projects.
Based on local data and input from relevant stakeholders and considering the support available from the HD2A Support Centers, applicants should propose projects likely to have a measurable and sustained impact on overdose and/or opioid-related outcomes, as relevant to their targeted element(s) of the Overdose Prevention Strategy, i.e., primary prevention, harm reduction, treatment of opioid use disorder, and recovery support. These projects should integrate data-driven decision making informed by new or improved partnerships with relevant organizational components (for Single System projects) or stakeholders (for Cross-Sector projects).
Examples of possible data-driven activities for Innovation Projects may include, but are not limited to:
- Use of rapid-cycle testing to support the implementation of an evidence-based practice in OUD care, effective pain-management, or primary prevention not previously in available or provide access through referrals
- Creation of cross-sector databases to support interdisciplinary patient care teams and successful referrals to relevant services (e.g., prevention, treatment, harm reduction, recovery, etc.)
- Development of data dashboards and community coalitions to identify and prioritize prevention or treatment service delivery gaps
- Improve measurement-based care of opioid use disorder
- Improve measurement-based pain assessment and management with evidence-based treatments to reduce unnecessary opioid prescribing
- Improve identification and linkage to primary prevention services or treatment for individuals with opioid use disorder (e.g., through use of consultation-liaison services)
- Inform clinician prescribing for effective pain management, referral to prevention services, or treatment for opioid use disorder, integrating data from Prescription Drug Monitoring Programs and patient-reported outcomes into the electronic health record
- Improve the delivery of treatment services using industry or protected data that are not currently accessible
Phases of the Award & Milestones
This funding opportunity uses a R61/R33 Exploratory/Developmental Phased Award mechanism. Support will be provided for a maximum of 5 years, which includes initial support of up to 2 years of the R61 phase, followed by up to 4 years of support for the R33 phase upon successfully meeting R61 milestones.
The R61 phase is a planning phase that can be up to two years and will support activities that demonstrate feasibility of bringing together relevant stakeholders and data sources to support the proposed activities. It is expected that work during this phase will largely focus on issues related to (1) improving aspects of data necessary to support R33 phase activities (e.g., quality, timeliness, relevance, availability, interoperability, linkage and integration, privacy issues, etc.), (2) stakeholder engagement to ensure feasibility, buy-in, sustainability, scalability, etc., and (3) pilot testing the ability to use data to inform actions. Applications must delineate milestones that signify the completion of major elements necessary to support a larger scale project in the second phase (e.g., accessing or improving timeliness of a specific dataset; establishing Memoranda of Understanding [MOU] to facilitate data sharing or working relationships with key stakeholders; establishing processes to use data in real-time; building dashboards, etc.). Applications are strongly encouraged to include contingency plans to proactively confront potential delays in meeting the milestones.
For transition to the R33 phase, recipients must submit the transition package no less than two months before the completion of the R61 phase. The transition plan should include the R61 progress report describing in detail the progress towards the R61 milestones and a description of how research proposed for the R33 phase will be supported by the completion of the R61 phase milestones. These materials will be evaluated by NIH program staff to determine if the milestones were met.
R33 funding decisions will be based on the original R61/R33 peer review recommendations, successful completion of transition milestones, any proposed changes to the R33 research based on R61 findings, program priorities, and availability of funds. It is not expected that all applications will continue to the R33 phase.
The goal of the R61 phase of the award is to demonstrate capacity to bring together necessary data sources and stakeholders to engage in an action-oriented project in Phase 2 of the project. The primary objective of the R33 phase should be to either (1) develop data or methods that improve the timeliness, quality, accessibility, and usefulness of data to allow for faster and improved responses to address the overdose epidemic (Acceleration Projects), or (2) identify and fill service delivery gaps with evidence-based strategies and monitor improvements in overdose-related outcomes along the opioid care cascade (Innovation Projects). The objectives for the R33 phase should be based, at least in part, on findings from the R61 phase. The R33 phase of the project can include a clinical trial if appropriate to research questions and goals.
Pre-Application Consultation
Potential applicants are strongly encouraged to consult with NIDA Program staff early in the application development process. This early contact will provide an opportunity to discuss and clarify NIH policies and guidelines, including the scope of the project relative to the HEAL initiative mission and intent of this FOA. Inquiries may be emailed to: [email protected].
Special Considerations:
The following applications will be considered non-responsive and will not be reviewed:
- Applications that do not have direct relevance to one of the four pillars of the HHS Overdose Prevention Strategy
Further, applications that do not include a Timeline and Milestones plan will be considered non-compliant.
PI Meeting Attendance: The NIH HEAL Initiative will require a high level of coordination and sharing between investigators. It is expected that NIH HEAL Initiative recipients will cooperate and coordinate their activities after awards are made by participating in Program Director/Principal Investigator (PD/PI) meetings, including an annual HEAL Investigators Meeting, as well as other activities.
Diversity: In addition to scientific diversity, applicants should strive to address diversity in their team development plan. Research shows that diverse teams working together and capitalizing on innovative ideas and distinct perspectives outperform homogenous teams. Scientists and trainees from diverse backgrounds and life experiences bring different perspectives, creativity, and individual enterprise to address complex scientific problems. There are many benefits that flow from a diverse NIH-supported scientific workforce, including: fostering scientific innovation, enhancing global competitiveness, contributing to robust learning environments, improving the quality of the research, advancing the likelihood that underserved or health disparity populations participate in, and benefit from health research, and enhancing public trust. In spite of tremendous advancements in scientific research, information, educational, and research opportunities are not equally available to all. NIH encourages institutions to diversify their student and faculty populations to enhance the participation of individuals from groups that are underrepresented in the biomedical, clinical, behavioral, and social sciences. Please refer to Notice of NIH's Interest in Diversity NOT-OD-20-031 for more details.
Points to Consider Regarding Tobacco Industry Funding of NIDA Applicants: The National Advisory Council on Drug Abuse (NACDA) encourages NIDA and its grantees to consider the points it has set forth with regard to existing or prospective sponsored research agreements with tobacco companies or their related entities and the impact of acceptance of tobacco industry funding on NIDA's credibility and reputation within the scientific community. Please see (http://ww2.drugabuse.gov/about/organization/nacda/points-to-consider.html) for details.
Data Harmonization for Substance Abuse and Addiction via the PhenX Toolkit: NIDA strongly encourages investigators involved in human-subjects studies to employ a common set of tools and resources that will promote the collection of comparable data across studies and to do so by incorporating the measures from the Core and Specialty collections, which are available in the Substance Abuse and Addiction Collection of the PhenX Toolkit (www.phenxtoolkit.org). Please see NOT-DA-12-008 for further details.
Common Data Elements: The HEAL Clinical Pain Common Data Element (CDE) Initiative provides an unprecedented opportunity for the pain research community to access quality and meaningful data across pain conditions, populations, and multiple interventions. The HEAL CDE Initiative aims to facilitate cross-study comparisons, improve interpretability of findings for patient-reported outcomes, and improve the ability to compare results across trials to quantify the impact of interventions. For studies focused on pain management, projects will be required to use the HEAL Clinical Pain Core CDEs which include measures within 9 pain domains and are specific to either adult or pediatric populations and acute or chronic pain conditions. The domains include pain intensity, pain interference, physical functioning/quality of life, sleep, pain catastrophizing, depression, anxiety, treatment satisfaction, and a substance use screener (HEAL CDE Program). Studies that use additional pain screening tools must select from a comprehensive set coded through HEAL or submit their tools for coding to comply with HEAL pain data harmonization. Any outcome measures specific to clinical pain should be validated measures appropriate for the pain condition.
See Section VIII. Other Information for award authorities and regulations.
Investigators proposing NIH-defined clinical trials may refer to the Research Methods Resources website for information about developing statistical methods and study designs.
Grant: A support mechanism providing money, property, or both to an eligible entity to carry out an approved project or activity.
Resubmission
Applicants with research previously reviewed under RFA-DA-22-051 may submit applications as resubmissions. Applicants with research previously reviewed under RFA-DA-22-044 and RFA-DA-22-045 may only submit applications as new submissions. Applications including research previously reviewed under RFA-DA-22-044 and RFA-DA-22-045 that are submitted as resubmissions will be returned without review.
The OER Glossary and the SF424 (R&R) Application Guide provide details on these application types. Only those application types listed here are allowed for this FOA.
Optional: Accepting applications that either propose or do not propose clinical trial(s).
NIH intends to commit $5 million in FY 2023 and the companion FOA RFA-DA-23-058 to fund 6-8 awards, pending availability of funds and receipt of a sufficient number of meritorious applications
Application budgets are not limited but need to reflect the actual needs of the proposed project. Unless well-justified, it is strongly recommended that applicants not request a budget of more than $350,000 in direct costs per year for the R61 phase and $750,000 in direct costs per year for the R33 phase.
The scope of the project should determine the project period for each phase. The maximum period of the combined R61 and R33 phases is 5 years, with 1 to 2 years for the R61 phase and up to 4 years for the R33 phase. The R61 is a milestone-driven planning phase, with possible transition to the implementation phase (R33). Only R61 projects that meet the scientific milestones and feasibility requirements will transition to the R33 phase. The R61/R33 application must be submitted as a single application, following the instructions described in this FOA.
NIH grants policies as described in the NIH Grants Policy Statement will apply to the applications submitted and awards made from this FOA.
1. Eligible Applicants
Higher Education Institutions
- Public/State Controlled Institutions of Higher Education
- Private Institutions of Higher Education
The following types of Higher Education Institutions are always encouraged to apply for NIH support as Public or Private Institutions of Higher Education:
- Hispanic-serving Institutions
- Historically Black Colleges and Universities (HBCUs)
- Tribally Controlled Colleges and Universities (TCCUs)
- Alaska Native and Native Hawaiian Serving Institutions
- Asian American Native American Pacific Islander Serving Institutions (AANAPISIs)
Nonprofits Other Than Institutions of Higher Education
- Nonprofits with 501(c)(3) IRS Status (Other than Institutions of Higher Education)
- Nonprofits without 501(c)(3) IRS Status (Other than Institutions of Higher Education)
For-Profit Organizations
- Small Businesses
- For-Profit Organizations (Other than Small Businesses)
Local Governments
- State Governments
- County Governments
- City or Township Governments
- Special District Governments
- Indian/Native American Tribal Governments (Federally Recognized)
- Indian/Native American Tribal Governments (Other than Federally Recognized)
Federal Government
- Eligible Agencies of the Federal Government
- U.S. Territory or Possession
Other
- Independent School Districts
- Public Housing Authorities/Indian Housing Authorities
- Native American Tribal Organizations (other than Federally recognized tribal governments)
- Faith-based or Community-based Organizations
- Regional Organizations
Non-domestic (non-U.S.) Entities (Foreign Institutions) are not eligible to apply.
Non-domestic (non-U.S.) components of U.S. Organizations are not eligible to apply.
Foreign components, as defined in the NIH Grants Policy Statement, are allowed.
Applicant Organizations
Applicant organizations must complete and maintain the following registrations as described in the SF 424 (R&R) Application Guide to be eligible to apply for or receive an award. All registrations must be completed prior to the application being submitted. Registration can take 6 weeks or more, so applicants should begin the registration process as soon as possible. The NIH Policy on Late Submission of Grant Applications states that failure to complete registrations in advance of a due date is not a valid reason for a late submission.
- System for Award Management (SAM) Applicants must complete and maintain an active registration, which requires renewal at least annually. The renewal process may require as much time as the initial registration. SAM registration includes the assignment of a Commercial and Government Entity (CAGE) Code for domestic organizations which have not already been assigned a CAGE Code.
- NATO Commercial and Government Entity (NCAGE) Code Foreign organizations must obtain an NCAGE code (in lieu of a CAGE code) in order to register in SAM.
- Unique Entity Identifier (UEI)- A UEI is issued as part of the SAM.gov registration process. The same UEI must be used for all registrations, as well as on the grant application.
- eRA Commons - Once the unique organization identifier is established, organizations can register with eRA Commons in tandem with completing their full SAM and Grants.gov registrations; all registrations must be in place by time of submission. eRA Commons requires organizations to identify at least one Signing Official (SO) and at least one Program Director/Principal Investigator (PD/PI) account in order to submit an application.
- Grants.gov Applicants must have an active SAM registration in order to complete the Grants.gov registration.
Program Directors/Principal Investigators (PD(s)/PI(s))
All PD(s)/PI(s) must have an eRA Commons account. PD(s)/PI(s) should work with their organizational officials to either create a new account or to affiliate their existing account with the applicant organization in eRA Commons. If the PD/PI is also the organizational Signing Official, they must have two distinct eRA Commons accounts, one for each role. Obtaining an eRA Commons account can take up to 2 weeks.
Any individual(s) with the skills, knowledge, and resources necessary to carry out the proposed research as the Program Director(s)/Principal Investigator(s) (PD(s)/PI(s)) is invited to work with his/her organization to develop an application for support. Individuals from diverse backgrounds, including underrepresented racial and ethnic groups, individuals with disabilities, and women are always encouraged to apply for NIH support. See, Reminder: Notice of NIH's Encouragement of Applications Supporting Individuals from Underrepresented Ethnic and Racial Groups as well as Individuals with Disabilities, NOT-OD-22-019.
For institutions/organizations proposing multiple PDs/PIs, visit the Multiple Program Director/Principal Investigator Policy and submission details in the Senior/Key Person Profile (Expanded) Component of the SF424 (R&R) Application Guide.
2. Cost Sharing
This FOA does not require cost sharing as defined in the NIH Grants Policy Statement.
3. Additional Information on Eligibility
Number of Applications
Applicant organizations may submit more than one application, provided that each application is scientifically distinct.
The NIH will not accept duplicate or highly overlapping applications under review at the same time, per 2.3.7.4 Submission of Resubmission Application. This means that the NIH will not accept:
- A new (A0) application that is submitted before issuance of the summary statement from the review of an overlapping new (A0) or resubmission (A1) application.
- A resubmission (A1) application that is submitted before issuance of the summary statement from the review of the previous new (A0) application.
- An application that has substantial overlap with another application pending appeal of initial peer review (see 2.3.9.4 Similar, Essentially Identical, or Identical Applications).
1. Requesting an Application Package
The application forms package specific to this opportunity must be accessed through ASSIST, Grants.gov Workspace or an institutional system-to-system solution. Links to apply using ASSIST or Grants.gov Workspace are available in Part 1 of this FOA. See your administrative office for instructions if you plan to use an institutional system-to-system solution.
2. Content and Form of Application Submission
It is critical that applicants follow the instructions in the Research (R) Instructions in the SF424 (R&R) Application Guide except where instructed in this funding opportunity announcement to do otherwise. Conformance to the requirements in the Application Guide is required and strictly enforced. Applications that are out of compliance with these instructions may be delayed or not accepted for review.
Letter of Intent
Although a letter of intent is not required, is not binding, and does not enter into the review of a subsequent application, the information that it contains allows IC staff to estimate the potential review workload and plan the review.
By the date listed in Part 1. Overview Information, prospective applicants are asked to submit a letter of intent that includes the following information:
- Descriptive title of proposed activity
- Name(s), address(es), and telephone number(s) of the PD(s)/PI(s)
- Names of other key personnel
- Participating institution(s)
- Number and title of this funding opportunity
The letter of intent should be sent to: [email protected]
All page limitations described in the SF424 Application Guide and the Table of Page Limits must be followed.
The following section supplements the instructions found in the SF424 (R&R) Application Guide and should be used for preparing an application to this FOA.
All instructions in the SF424 (R&R) Application Guide must be followed.
All instructions in the SF424 (R&R) Application Guide must be followed.
All instructions in the SF424 (R&R) Application Guide must be followed, with the following additional instructions:
Timeline & Milestone Plan (Required - 2 page maximum):
Applicants should include a Timeline and Milestone Plan, clearly specifying proposed milestones and when those milestones are expected to be achieved. Milestones for both phases should be specified, though it is expected that R33 milestones may change based on results from the R61 phase for awards that transition to the R33 phase.
Stakeholder Engagement Plan (Required 2 page maximum):
Applications should include detailed plans for engaging key stakeholders, including patients, families, providers, payers, and community leaders, as appropriate to the specific goals of their study.
All instructions in the SF424 (R&R) Application Guide must be followed, with the following additional instructions:
Applicants are strongly encouraged to include relevant staff from partnered organizations as part of key personnel.
R&R Budget
All instructions in the SF424 (R&R) Application Guide must be followed, with the following additional instructions:
Meetings and Travel: Applicants should assume that all meetings referenced throughout this FOA will be held virtually unless otherwise specified.
HEAL D2A Program Meeting(s): A virtual kickoff meeting will be held within 1 month of awards being made. PI(s) and other personnel will be expected to participate in baseline needs assessment meetings with the 3 HEAL Data2Action coordinating components during the first year of the award, as well as mid-project needs assessment meetings if successfully transitioning to the R33 phase, and an end-of-project evaluation in the last year of the award.
Budgets should include funds for travel for up to 3 people to participate in 3-day in-person HEAL Data2Action meetings to discuss findings two times over the course of the award, once within the first year and once in the middle of the project period in the Washington DC area.
HEAL Investigators Meeting: For budgeting purposes, include travel costs to support the attendance of one PD/PI (one person) at a 2-day, in-person HEAL Investigators meeting in the Washington DC area, annually for the duration of the award.
All instructions in the SF424 (R&R) Application Guide must be followed.
All instructions in the SF424 (R&R) Application Guide must be followed.
All instructions in the SF424 (R&R) Application Guide must be followed, with the following additional instructions:
Specific Aims:
In the single page attachment allowed for the specific aims, applicants should provide an overview of the overarching research question of interest as well as include clearly marked headers for R61 Specific Aims and R33 Specific Aims with brief descriptions of the aims specific to each phase of the study.
Research Strategy:
Section A: Research Strategy
The Research Strategy should be organized in a manner that will facilitate peer review. The body of the application should present an overview of the state of the science, current status and relevance of the proposed activities, and consideration of long-term sustainability and scalability of the proposed efforts.
The following criteria should be addressed:
Significance:The R61 and R33 should coherently address a single set of research questions and goals, with the R61 phase establishing feasibility and necessary data infrastructure for the R33 phase. Given this tight integration, only one Significance section is needed.
Applications should articulate the overall goals and scientific approach that will guide the proposed efforts, clearly specifying the problem that is trying to be solved and articulating the following:
- Targeted systems and/or stakeholders & the targeted actions that are under the control of these systems/stakeholders, including a discussion of the relevance of these issues to organizations, systems, or communities other than those participating in the study.
- Targeted outcomes, including relevance to the four pillars in the HHS Overdose Prevention Strategy. If overdose-related morbidity and mortality outcomes are not included, applications should specifically address how the targeted outcomes are related to overdose and/or opioid-related morbidity and mortality. Applicants should address ability to assess burden, trends, and impacts at broader systems and community levels.
- Pain management outomes. Studies designed to implement effective pain management strategies should include a plan to collect the HEAL Clinical Pain Common Data Elements (CDE) from participants. The HEAL CDE Initiative aims to facilitate cross-study comparisons, improve interpretability of findings for patient-reported outcomes, and improves the ability to compare results across trials to quantify the impact of interventions. For studies focused on pain management, projects will be required to use the HEAL Clinical Pain Core CDEs which include measures within 9 pain domains and are specific to either adult or pediatric populations and acute or chronic pain conditions. The domains include pain intensity, pain interference, physical functioning/quality of life, sleep, pain catastrophizing, depression, anxiety, treatment satisfaction, and a substance use screener (HEAL CDE Program). Studies that use additional pain screening tools must select from a comprehensive set coded through HEAL or submit their tools for coding to comply with HEAL pain data harmonization. Any outcome measures specific to clinical pain should be validated measures appropriate for the pain condition.
- Clear justification for why addressing the specific data-related gaps or inefficiencies should be able to inform epidemiology and/or lead to improvements in service delivery, including issues of sustainability and scalability.
- Discussion of other efforts funded by other federal, state, or local funders, including settlement funds, with special attention to the relevance of these efforts for sustainability and scalability. Applicants are strongly encouraged to leverage and build on other efforts currently active in the targeted systems/communities.
- Quantify the scope of the expected impact of the proposed project, e.g., quantify the number of patients in the relevant geographic area (state, community, etc.) or targeted system where outcomes would be demonstrated.
- Supporting scientific justification.
Innovation: Given this tight integration of the R61/R33 phases, only one Innovation section is needed. The Innovation section should explain how the proposed project, if successful, would lead to innovations that could improve the utilization of data to support and sustain action-oriented approaches to reduce overdoses or improve opioid-relevant outcomes not just in the targeted system or community, but how these findings might be more broadly applicable.
Preliminary data is not required for HD2A R61 grants nor is it required that teams have worked together previously. The phased award approach allows for earlier stage high risk/high reward projects. However, applications without preliminary data should have a strong scientific premise and establish a strong rationale for how solving the challenges outlined in the application would improve outcomes relevant to overdoses and/or opioid-related morbidity and mortality.
Approach: The application should contain separate Approach sections for the R61 and R33 phases, as described below. It is not necessary to repeat any information or details in the R33 section that are described in the R61 section. Applicants should specify which Priority they are responding to in their applications - (1) Acceleration or (2) Innovation. Applications must include a Timeline & Milestone plan and a Stakeholder Engagement Plan as attachments as described in the SF424(R&R) Other Project Information. The approach sections may reference this attachment and should limit what is repeated from this attachment, except where necessary for clarity.
R61 (Phase 1) Approach:
The R61 Approach section application must include milestones that are expected to be achieved by the end of the R61 phase. Milestones should be specific, quantifiable, and scientifically justified; they should not be simply a restatement of the specific aims for the R61 phase.
All projects should include the following in the R61 approach section:
- Specify the data-related gaps or inefficiencies being targeted
- Plans for stakeholder engagement, including, where relevant, engagement with patients
- Plans to understand and address issues of equity in service delivery
- Plans to enhance the likelihood that innovations developed in the application will be sustained, including engaging relevant stakeholders
- Length of R61 phase and specification of relevant milestones (see below)
- Contingency plans if milestones cannot be achieved
Examples of Milestones for the R61 Phase:
- Fully executed MOUs, letters of support, and data sharing agreements, as relevant to the goals of the study, from partnering departments, agencies or stakeholders
- Data infrastructure milestones necessary to launch the R33 phase of the project (e.g., quality, timeliness, relevance, availability, interoperability, integration, etc.)
- Demonstration of active engagement and partnership with key entities and stakeholders (e.g., formation of trans-department or trans-agency change teams)
- If preliminary data was not included in original application, preliminary data demonstrating feasibility of R33 phase must be included.
For applications where there is no preliminary data or where new partnerships are proposed, applicants should be especially attentive to proposing milestones that will help establish the feasibility of their proposed R33 project.
R33 (Phase 2) Approach
Although the Research Strategy for the R33 Phase is expected to be broad and flexible due to the nature of the explorative research in the R61 Phase, the research strategy for the R33 phase of the award should be described in enough detail for reviewers to evaluate the merit of this component of the application, based on anticipated results.
The proposed milestones for the R33 phase may be revised based on activities during the R61 planning phase. In the event of an award, the PD/PI and NIH staff will negotiate proposed changes and a list of appropriate milestones for each year of support.
The R33 phase may include a clinical trial if appropriate for the research questions and study design, but other designs may be appropriate and acceptable depending on research goals. Applications that propose a clinical trial in the R33 phase should include relevant information for the proposed clinical trial in the clinical trial attachment. Research methods and designs are expected to be scientifically rigorous, and designs should match the research questions posed. As with milestones, the overall design of the R33 may be modified based on findings from the R61 phase, if appropriate. Any such modifications must be discussed in advance with NIH program staff and would include discussions of relevant changes to the proposed milestones.
Section B: Interaction with Data2Action Supportive Infrastructure
Awards made under this FOA are part of a coordinated initiative and as such will have access to a robust set of supportive infrastructure resources. Applications should demonstrate their capacity to do the proposed work, but it is also expected that additional needs could arise. The supportive infrastructure being funded under the HD2A program is meant to anticipate some of these additional needs. Specifically, the HD2A program will provide applicants with supportive infrastructure in the following areas:
- Data infrastructure support
- Data infrastructure, tools, resource support & coordination
- Measurement & analytic support
- Data-relevant training and resource support (e.g., access to visualization tools, etc.)
- Data modernization support
- Economic & modeling support
- Predictive, simulation, geospatial, and cost modeling to aid in forecasting service needs
- Costing tools to estimate costs of implemented changes and their outcomes
- Consultation on the use of behavioral economic strategies to promote practice change
- Research adoption support
- Curated catalog of evidence-based practices and implementation strategies that may be deployed to support the adoption of new approaches to addressing pain and substance use disorder
- Consultation on selection of implementation options in the absence of a strong evidence base
- Guidance with the development of logic models and outcome measures
Applications should include a section describing how these resources could be used to extend the work proposed and describe interest and capacity in interfacing with these resources, specifically addressing:
- Expected support needed from the Data Infrastructure Support Center and how those resources will enable the acquisition, combination, and/or analysis of local data to drive decisions
- Expected support needed from the Research Adoption Support Center, e.g., to identify potential evidence-based practices and implementation strategies to be deployed to address identified needs
- How the project might work with the Economics and Modeling Resource Center, e.g., to forecast patient population needs, compare cost and cost-benefit associated with different implementation options, or to model potential locations for new service delivery sites
- Commitment to engaging in a needs assessment conducted by the Centers to identify where there are relevant and appropriate opportunities to receive support
At a minimum, applicants should expect to engage in a virtual kickoff meeting with all recipients of the HEAL Data2Action program and an in-person update meeting toward the end of year 1. In addition, all Innovation and Acceleration Projects will be expected to participate in needs assessments meetings with relevant Resource Centers in the first year of the award, a mid-course needs assessment upon transition to the R33 phase, and an end-of-project evaluation in the last year of the award. Innovation Project grantees should also expect to participate in regular check-ins with NIDA program staff.
Letters of Support: Include letters of support/agreement for any collaborative arrangements, subcontracts or consultants. For activities to be conducted at an institution other than the applicant institution, a letter of assurance or comparable documentation, signed by the collaborator as well as the institutional officials, must be submitted with the application.
Applicants should include relevant letters of support from targeted systems or stakeholders. Where relationships with relevant systems or stakeholders do not exist or are not yet fully formalized, applicants should include formalizing these relationships as a milestone.
Resource Sharing Plan: Individuals are required to comply with the instructions for the Resource Sharing Plans as provided in the SF424 (R&R) Application Guide.
All applications, regardless of the amount of direct costs requested for any one year, must address a Data Sharing Plan.
It is expected that most projects will use existing and/or administrative data that where there might be restrictions to sharing or limitations to the ability to collect new or different data. Even so, applicants should share when possible. Data sharing plans should be clearly described including any limitations on data sharing that may affect ability to comply with the HEAL Initiative Data Sharing Policy as described below.
Data sharing plans should align with the HEAL Initiative Public Access and Data Sharing Policy as described below.
NIH intends to maximize the impact of HEAL Initiative-supported projects through broad and rapid data sharing. Consistent with the HEAL Initiative Public Access and Data Sharing Policy (https://heal.nih.gov/about/public-access-data), all applications, regardless of the amount of direct costs requested for any one year, are required to include a Data Management and Sharing Plan outlining how scientific data and any accompanying metadata will be managed and shared. The plan should describe data types, file formats, submission timelines, and standards used in collecting or processing the data. It is expected that data generated by HEAL Initiative-funded projects will be submitted to study-appropriate domain-specific or generalist repositories in consultation with the HEAL Data Stewardship Group to ensure the data is accessible via the HEAL Initiative Data Ecosystem. Guidelines for complying with the HEAL Public Access and Data Sharing Policy can be found at https://heal.nih.gov/data/complying-heal-data-sharing-policy. Resources and tools to assist with data related activities can be found at https://www.healdatafair.org/.
The Data Management and Sharing Plan represents a commitment by the institution (and its subcontractors, as applicable) to support and abide by the plan. Prior to funding, the approved Data Management and Sharing Plan will be a condition of the award. Guidance for writing and examples of data management and sharing plans can be found on the NIH website: Writing a Data Management & Sharing Plan | Data Sharing (nih.gov).
To maximize discoverability and value of HEAL datasets and studies, and facilitate data integration and collaboration, applications submitted in response to this FOA are strongly encouraged to incorporate standards and resources where applicable:
- Applicants are encouraged to ensure that data collected by the study conform to Findable, Accessible, Interoperable, and Reusable (FAIR) principles.
- Applicants are specifically encouraged to incorporate into their planning, an alignment with the guidelines, principles and recommendations developed by the HEAL Data Ecosystem, including but not limited to preparing data to store in selected specified repositories, applying minimal metadata standards, use of core HEAL Clinical Data Elements (CDEs, https://heal.nih.gov/data/common-data-elements), and other necessary requirements to prepare data to connect to the HEAL Data Ecosystem.
- All new HEAL clinical pain studies are required to submit their case-report forms/questionnaires to the HEAL Clinical Data Elements (CDE) Program. The program will create the CDE files containing standardized variable names, responses, coding, and other information. The program will also format the case-report forms in a standardized way that is compliant with accessibility standards under Section 508 of the Rehabilitation Act of 1973 (29 U.S.C 794 (d)), which require[s] Federal agencies to make their electronic and information technology accessible to people with disabilities. HEAL Initiative clinical studies that are using copyrighted questionaries are required to obtain licenses for use prior to initiating data collection. Licenses must be shared with the HEAL CDE team and the program officer prior to use of copyrighted materials. For additional information, visit the HEAL CDE Program.
- To the extent possible, HEAL awardees are expected to integrate broad data sharing consent language into their informed consent forms and align study consent language with data access and re-use requirements as defined by the repository HEAL investigators select to store their HEAL data long term.
The NIH notices referenced below provide additional NIH guidance that should be considered in developing a strong data management and sharing plan. The list is instructive but not comprehensive.
- NIH has provided guidance around selecting a repository for data generated by NIH-supported research and has developed desirable characteristics for all data repositories (NOT-OD-21-016).
- NIH encourages the use of data standards including the PhenX Toolkit (www.phenxtoolkit.org) (for example, see NOT-DA-12-008, NOT-MH-15-009).
- Data should be organized according to a standard model that is widely accepted within the field. An example for the clinical research studies would be the OMOP Common Data Model, which has also been successfully adapted for use with observational (including survey) studies more generally. In addition, the HL7 FHIR (Fast Healthcare Interoperability Resources) standard (NOT-OD-19-122) may facilitate the flow of data with EHR-based datasets, tools, and applications.
- NIH encourages clinical research programs and researchers to adopt and use the standardized set of data classes, data elements, and associated vocabulary standards specified in the United States Core Data for Interoperability (USCDI)standards, as they are applicable (NOT-OD-20-146). Use of the USCDI can complement the FHIR standard and enable researchers to leverage structured EHR data for research and enable discovery. In addition to USCDI, OMOP, and FHIR standards for enhanced interoperability, investigators and data centers should align their data collection and management practices with recommended guidance emerging from the HEAL CDE and Data Ecosystem programs.
Recipients conducting research that includes collection of genomic data should incorporate requirements under the NIH Genomic Data Sharing Policy (NOT-OD-14-124, NOT-OD-15-086).
When involving human subjects research, clinical research, and/or NIH-defined clinical trials (and when applicable, clinical trials research experience) follow all instructions for the PHS Human Subjects and Clinical Trials Information form in the SF424 (R&R) Application Guide, with the following additional instructions:
If you answered Yes to the question Are Human Subjects Involved? on the R&R Other Project Information form, you must include at least one human subjects study record using the Study Record: PHS Human Subjects and Clinical Trials Information form or Delayed Onset Study record.
Study Record: PHS Human Subjects and Clinical Trials Information
All instructions in the SF424 (R&R) Application Guide must be followed.
Delayed Onset Study
Note: Delayed onset does NOT apply to a study that can be described but will not start immediately (i.e., delayed start).All instructions in the SF424 (R&R) Application Guide must be followed.
All instructions in the SF424 (R&R) Application Guide must be followed.
3. Unique Entity Identifier and System for Award Management (SAM)
See Part 1. Section III.1 for information regarding the requirement for obtaining a unique entity identifier and for completing and maintaining active registrations in System for Award Management (SAM), NATO Commercial and Government Entity (NCAGE) Code (if applicable), eRA Commons, and Grants.gov.
Part I. Overview Information contains information about Key Dates and times. Applicants are encouraged to submit applications before the due date to ensure they have time to make any application corrections that might be necessary for successful submission. When a submission date falls on a weekend or Federal holiday, the application deadline is automatically extended to the next business day.
Organizations must submit applications to Grants.gov (the online portal to find and apply for grants across all Federal agencies). Applicants must then complete the submission process by tracking the status of the application in the eRA Commons, NIH’s electronic system for grants administration. NIH and Grants.gov systems check the application against many of the application instructions upon submission. Errors must be corrected and a changed/corrected application must be submitted to Grants.gov on or before the application due date and time. If a Changed/Corrected application is submitted after the deadline, the application will be considered late. Applications that miss the due date and time are subjected to the NIH Policy on Late Application Submission.
Applicants are responsible for viewing their application before the due date in the eRA Commons to ensure accurate and successful submission.
Information on the submission process and a definition of on-time submission are provided in the SF424 (R&R) Application Guide.
5. Intergovernmental Review (E.O. 12372)
This initiative is not subject to intergovernmental review.
All NIH awards are subject to the terms and conditions, cost principles, and other considerations described in the NIH Grants Policy Statement.
Pre-award costs are allowable only as described in the NIH Grants Policy Statement.
Applications must be submitted electronically following the instructions described in the SF424 (R&R) Application Guide. Paper applications will not be accepted.
Applicants must complete all required registrations before the application due date. Section III. Eligibility Information contains information about registration.
For assistance with your electronic application or for more information on the electronic submission process, visit How to Apply Application Guide. If you encounter a system issue beyond your control that threatens your ability to complete the submission process on-time, you must follow the Dealing with System Issues guidance. For assistance with application submission, contact the Application Submission Contacts in Section VII.
Important reminders:
All PD(s)/PI(s) must include their eRA Commons ID in the Credential fieldof the Senior/Key Person Profile form. Failure to register in the Commons and to include a valid PD/PI Commons ID in the credential field will prevent the successful submission of an electronic application to NIH. See Section III of this FOA for information on registration requirements.
The applicant organization must ensure that the unique entity identifier provided on the application is the same identifier used in the organization’s profile in the eRA Commons and for the System for Award Management. Additional information may be found in the SF424 (R&R) Application Guide.
See more tips for avoiding common errors.
Upon receipt, applications will be evaluated for completeness and compliance with application instructions by the Center for Scientific Review and responsiveness by NIDA, NIH. Applications that are incomplete, non-compliant and/or nonresponsive will not be reviewed.
Applicants are required to follow the instructions for post-submission materials, as described in the policy. Any instructions provided here are in addition to the instructions in the policy.
1. Criteria
Only the review criteria described below will be considered in the review process. Applications submitted to the NIH in support of the NIH mission are evaluated for scientific and technical merit through the NIH peer review system.
A proposed Clinical Trial application may include study design, methods, and intervention that are not by themselves innovative but address important questions or unmet needs. Additionally, the results of the clinical trial may indicate that further clinical development of the intervention is unwarranted or lead to new avenues of scientific investigation.
Overall Impact
Reviewers will provide an overall impact score to reflect their assessment of the likelihood for the project to exert a sustained, powerful influence on the research field(s) involved, in consideration of the following review criteria and additional review criteria (as applicable for the project proposed).
Scored Review Criteria
Reviewers will consider each of the review criteria below in the determination of scientific merit and give a separate score for each. An application does not need to be strong in all categories to be judged likely to have major scientific impact. For example, a project that by its nature is not innovative may be essential to advance a field.
Significance
Does the project address an important problem or a critical barrier to progress in the field? Is the prior research that serves as the key support for the proposed project rigorous? If the aims of the project are achieved, how will scientific knowledge, technical capability, and/or clinical practice be improved? How will successful completion of the aims change the concepts, methods, technologies, treatments, services, or preventative interventions that drive this field?
For Priority 1 Acceleration Projects: Are the expectations of the project realistic and in line with the planned efforts? Does the proposed method or algorithm have the potential to be widely adopted by the relevant research and/or public health community? Do the proposed data or methods have the potential to improve the timeliness, quality, accessibility, or usefulness of existing data ecosystems to allow for faster and improved responses to address the overdose epidemic?
For Priority 2 Innovation Projects: Does the proposed study propose a project that addresses a critical data-related gap or inefficiency that if addressed, could lead to significant improvements in service delivery? Does the application address issues of sustainability and scalability? Does the application build on relevant efforts in the targeted system or community? Can adequate assessment of impact at the systems or community level be expected?
In addition, for applications involving clinical trials
Are the scientific rationale and need for a clinical trial to test the proposed hypothesis or intervention well supported by preliminary data, clinical and/or preclinical studies, or information in the literature or knowledge of biological mechanisms? For trials focusing on clinical or public health endpoints, is this clinical trial necessary for testing the safety, efficacy or effectiveness of an intervention that could lead to a change in clinical practice, community behaviors or health care policy? For trials focusing on mechanistic, behavioral, physiological, biochemical, or other biomedical endpoints, is this trial needed to advance scientific understanding?
Investigator(s)
Are the PD(s)/PI(s), collaborators, and other researchers well suited to the project? If Early Stage Investigators or those in the early stages of independent careers, do they have appropriate experience and training? If established, have they demonstrated an ongoing record of accomplishments that have advanced their field(s)? If the project is collaborative or multi-PD/PI, do the investigators have complementary and integrated expertise; are their leadership approach, governance, and organizational structure appropriate for the project?
For Priority 1 Acceleration Projects: Do the scientific background and record of the PD(s)/PI(s) or any collaborators establish a strong record of developing data, approaches, and methods that can be applied to the areas of substance use or related field? Does the application include any collaborators who are the stakeholders/end-users of the product proposed? As appropriate to the proposed design, are key partners included as co-investigators and/or collaborators?
For Priority 2 Innovation Projects: As appropriate to the proposed design, are key partners included as co-investigators and/or collaborators?
In addition, for applications involving clinical trials
With regard to the proposed leadership for the project, do the PD/PI(s) and key personnel have the expertise, experience, and ability to organize, manage and implement the proposed clinical trial and meet milestones and timelines? Do they have appropriate expertise in study coordination, data management and statistics? For a multicenter trial, is the organizational structure appropriate and does the application identify a core of potential center investigators and staffing for a coordinating center?
Innovation
Does the application challenge and seek to shift current research or clinical practice paradigms by utilizing novel theoretical concepts, approaches or methodologies, instrumentation, or interventions? Are the concepts, approaches or methodologies, instrumentation, or interventions novel to one field of research or novel in a broad sense? Is a refinement, improvement, or new application of theoretical concepts, approaches or methodologies, instrumentation, or interventions proposed?
For Priority 1 Acceleration Projects: Is there innovation either in the data or method products developed or in how the data or method products is taken from one field and applied in another? Will the proposed data or method products offer new possibilities for substance use research relative to those currently available?
For Priority 2 Innovation Projects: Does the proposed project have the potential to lead to innovations that could improve the utilization of data to support and sustain action-oriented approaches to reduce overdoses or improve opioid-relevant outcomes not just in the targeted system or community, but more broadly?
In addition, for applications involving clinical trials
Does the design/research plan include innovative elements, as appropriate, that enhance its sensitivity, potential for information or potential to advance scientific knowledge or clinical practice?
Approach
Are the overall strategy, methodology, and analyses well-reasoned and appropriate to accomplish the specific aims of the project? Have the investigators included plans to address weaknesses in the rigor of prior research that serves as the key support for the proposed project? Have the investigators presented strategies to ensure a robust and unbiased approach, as appropriate for the work proposed? Are potential problems, alternative strategies, and benchmarks for success presented? If the project is in the early stages of development, will the strategy establish feasibility and will particularly risky aspects be managed? Have the investigators presented adequate plans to address relevant biological variables, such as sex, for studies in vertebrate animals or human subjects?
If the project involves human subjects and/or NIH-defined clinical research, are the plans to address 1) the protection of human subjects from research risks, and 2) inclusion (or exclusion) of individuals on the basis of sex/gender, race, and ethnicity, as well as the inclusion or exclusion of individuals of all ages (including children and older adults), justified in terms of the scientific goals and research strategy proposed?
For Priority 1 Acceleration & Priority 2 Innovation Projects: Are the milestones for the R61 phase well specified? Does the plan include well thought out plans for stakeholder engagement and patient engagement? Does the application employ a public health approach of data to action? Does the application take issues of equity into consideration? Does the length of the R61 phase seem appropriate relevant for the scope of work proposed? Are plans for the R33 phase well-articulated, including specification of research questions? Do the plans for the R33 phase build in a logical way on the R61 phase? Is there a well-articulated data sharing plan? Is this plan reasonable? Does the application show a well-thought-out consideration for how it might take advantage of the infrastructure and resources offered through the HD2A program? Does the application include sufficient resources dedicated to interfacing with other elements of the HD2A program? Do the design and methods allow for an understanding of burden, trends, and potential impact at the systems and community level?
In addition, for applications involving clinical trials
Does the application adequately address the following, if applicable
Study Design
Is the study design justified and appropriate to address primary and secondary outcome variable(s)/endpoints that will be clear, informative and relevant to the hypothesis being tested? Is the scientific rationale/premise of the study based on previously well-designed preclinical and/or clinical research? Given the methods used to assign participants and deliver interventions, is the study design adequately powered to answer the research question(s), test the proposed hypothesis/hypotheses, and provide interpretable results? Is the trial appropriately designed to conduct the research efficiently? Are the study populations (size, gender, age, demographic group), proposed intervention arms/dose, and duration of the trial, appropriate and well justified?
Are potential ethical issues adequately addressed? Is the process for obtaining informed consent or assent appropriate? Is the eligible population available? Are the plans for recruitment outreach, enrollment, retention, handling dropouts, missed visits, and losses to follow-up appropriate to ensure robust data collection? Are the planned recruitment timelines feasible and is the plan to monitor accrual adequate? Has the need for randomization (or not), masking (if appropriate), controls, and inclusion/exclusion criteria been addressed? Are differences addressed, if applicable, in the intervention effect due to sex/gender and race/ethnicity?
Are the plans to standardize, assure quality of, and monitor adherence to, the trial protocol and data collection or distribution guidelines appropriate? Is there a plan to obtain required study agent(s)? Does the application propose to use existing available resources, as applicable?
Data Management and Statistical Analysis
Are planned analyses and statistical approach appropriate for the proposed study design and methods used to assign participants and deliver interventions? Are the procedures for data management and quality control of data adequate at clinical site(s) or at center laboratories, as applicable? Have the methods for standardization of procedures for data management to assess the effect of the intervention and quality control been addressed? Is there a plan to complete data analysis within the proposed period of the award?
Environment
Will the scientific environment in which the work will be done contribute to the probability of success? Are the institutional support, equipment, and other physical resources available to the investigators adequate for the project proposed? Will the project benefit from unique features of the scientific environment, subject populations, or collaborative arrangements?
In addition, for applications involving clinical trials
If proposed, are the administrative, data coordinating, enrollment and laboratory/testing centers, appropriate for the trial proposed?
Does the application adequately address the capability and ability to conduct the trial at the proposed site(s) or centers? Are the plans to add or drop enrollment centers, as needed, appropriate?
If international site(s) is/are proposed, does the application adequately address the complexity of executing the clinical trial?
If multi-sites/centers, is there evidence of the ability of the individual site or center to: (1) enroll the proposed numbers; (2) adhere to the protocol; (3) collect and transmit data in an accurate and timely fashion; and, (4) operate within the proposed organizational structure?
Additional Review Criteria
As applicable for the project proposed, reviewers will evaluate the following additional items while determining scientific and technical merit, and in providing an overall impact score, but will not give separate scores for these items.
Study Timeline
Specific to applications involving clinical trials
Is the study timeline described in detail, taking into account start-up activities, the anticipated rate of enrollment, and planned follow-up assessment? Is the projected timeline feasible and well justified? Does the project incorporate efficiencies and utilize existing resources (e.g., CTSAs, practice-based research networks, electronic medical records, administrative database, or patient registries) to increase the efficiency of participant enrollment and data collection, as appropriate?
Are potential challenges and corresponding solutions discussed (e.g., strategies that can be implemented in the event of enrollment shortfalls)?
Protections for Human Subjects
For research that involves human subjects but does not involve one of the categories of research that are exempt under 45 CFR Part 46, the committee will evaluate the justification for involvement of human subjects and the proposed protections from research risk relating to their participation according to the following five review criteria: 1) risk to subjects, 2) adequacy of protection against risks, 3) potential benefits to the subjects and others, 4) importance of the knowledge to be gained, and 5) data and safety monitoring for clinical trials.
For research that involves human subjects and meets the criteria for one or more of the categories of research that are exempt under 45 CFR Part 46, the committee will evaluate: 1) the justification for the exemption, 2) human subjects involvement and characteristics, and 3) sources of materials. For additional information on review of the Human Subjects section, please refer to the Guidelines for the Review of Human Subjects.
Inclusion of Women, Minorities, and Individuals Across the Lifespan
When the proposed project involves human subjects and/or NIH-defined clinical research, the committee will evaluate the proposed plans for the inclusion (or exclusion) of individuals on the basis of sex/gender, race, and ethnicity, as well as the inclusion (or exclusion) of individuals of all ages (including children and older adults) to determine if it is justified in terms of the scientific goals and research strategy proposed. For additional information on review of the Inclusion section, please refer to the Guidelines for the Review of Inclusion in Clinical Research.
Vertebrate Animals
The committee will evaluate the involvement of live vertebrate animals as part of the scientific assessment according to the following criteria: (1) description of proposed procedures involving animals, including species, strains, ages, sex, and total number to be used; (2) justifications for the use of animals versus alternative models and for the appropriateness of the species proposed; (3) interventions to minimize discomfort, distress, pain and injury; and (4) justification for euthanasia method if NOT consistent with the AVMA Guidelines for the Euthanasia of Animals. Reviewers will assess the use of chimpanzees as they would any other application proposing the use of vertebrate animals. For additional information on review of the Vertebrate Animals section, please refer to the Worksheet for Review of the Vertebrate Animal Section.
Biohazards
Reviewers will assess whether materials or procedures proposed are potentially hazardous to research personnel and/or the environment, and if needed, determine whether adequate protection is proposed.
Resubmissions
For Resubmissions, the committee will evaluate the application as now presented, taking into consideration the responses to comments from the previous scientific review group and changes made to the project.
Renewals
Not Applicable.
Revisions
Not Applicable.
As applicable for the project proposed, reviewers will consider each of the following items, but will not give scores for these items, and should not consider them in providing an overall impact score.
Applications from Foreign Organizations
Not Applicable.
Select Agent Research
Reviewers will assess the information provided in this section of the application, including 1) the Select Agent(s) to be used in the proposed research, 2) the registration status of all entities where Select Agent(s) will be used, 3) the procedures that will be used to monitor possession use and transfer of Select Agent(s), and 4) plans for appropriate biosafety, biocontainment, and security of the Select Agent(s).
Resource Sharing Plans
Reviewers will comment on whether the following Resource Sharing Plans, or the rationale for not sharing the following types of resources, are reasonable: (1) Sharing Model Organisms; and (2) Genomic Data Sharing Plan (GDS).
Authentication of Key Biological and/or Chemical Resources:
For projects involving key biological and/or chemical resources, reviewers will comment on the brief plans proposed for identifying and ensuring the validity of those resources.
Budget and Period of Support
Reviewers will consider whether the budget and the requested period of support are fully justified and reasonable in relation to the proposed research.
2. Review and Selection Process
Applications will be evaluated for scientific and technical merit by (an) appropriate Scientific Review Group(s) convened by NIDA , in accordance with NIH peer review policy and procedures, using the stated review criteria. Assignment to a Scientific Review Group will be shown in the eRA Commons.
As part of the scientific peer review, all applications will receive a written critique.
Applications may undergo a selection process in which only those applications deemed to have the highest scientific and technical merit (generally the top half of applications under review) will be discussed and assigned an overall impact score.
Appeals of initial peer review will not be accepted for applications submitted in response to this FOA.
- Scientific and technical merit of the proposed project as determined by scientific peer review.
- Availability of funds.
- Relevance of the proposed project to program priorities.
3. Anticipated Announcement and Award Dates
After the peer review of the application is completed, the PD/PI will be able to access his or her Summary Statement (written critique) via the eRA Commons. Refer to Part 1 for dates for peer review, advisory council review, and earliest start date.
Information regarding the disposition of applications is available in the NIH Grants Policy Statement.
1. Award Notices
If the application is under consideration for funding, NIH will request "just-in-time" information from the applicant as described in the NIH Grants Policy Statement.
A formal notification in the form of a Notice of Award (NoA) will be provided to the applicant organization for successful applications. The NoA signed by the grants management officer is the authorizing document and will be sent via email to the recipient's business official.
Recipients must comply with any funding restrictions described in Section IV.5. Funding Restrictions. Selection of an application for award is not an authorization to begin performance. Any costs incurred before receipt of the NoA are at the recipient's risk. These costs may be reimbursed only to the extent considered allowable pre-award costs.
Any application awarded in response to this FOA will be subject to terms and conditions found on the Award Conditions and Information for NIH Grants website. This includes any recent legislation and policy applicable to awards that is highlighted on this website.
Individual awards are based on the application submitted to, and as approved by, the NIH and are subject to the IC-specific terms and conditions identified in the NoA.
ClinicalTrials.gov: If an award provides for one or more clinical trials. By law (Title VIII, Section 801 of Public Law 110-85), the "responsible party" must register and submit results information for certain applicable clinical trials on the ClinicalTrials.gov Protocol Registration and Results System Information Website (https://register.clinicaltrials.gov). NIH expects registration and results reporting of all trials whether required under the law or not. For more information, see https://grants.nih.gov/policy/clinical-trials/reporting/index.htm
Institutional Review Board or Independent Ethics Committee Approval: Recipient institutions must ensure that all protocols are reviewed by their IRB or IEC. To help ensure the safety of participants enrolled in NIH-funded studies, the recipient must provide NIH copies of documents related to all major changes in the status of ongoing protocols.
Data and Safety Monitoring Requirements: The NIH policy for data and safety monitoring requires oversight and monitoring of all NIH-conducted or -supported human biomedical and behavioral intervention studies (clinical trials) to ensure the safety of participants and the validity and integrity of the data. Further information concerning these requirements is found at http://grants.nih.gov/grants/policy/hs/data_safety.htm and in the application instructions (SF424 (R&R) and PHS 398).
Investigational New Drug or Investigational Device Exemption Requirements: Consistent with federal regulations, clinical research projects involving the use of investigational therapeutics, vaccines, or other medical interventions (including licensed products and devices for a purpose other than that for which they were licensed) in humans under a research protocol must be performed under a Food and Drug Administration (FDA) investigational new drug (IND) or investigational device exemption (IDE).
2. Administrative and National Policy Requirements
All NIH grant and cooperative agreement awards include the NIH Grants Policy Statement as part of the NoA. For these terms of award, see the NIH Grants Policy Statement Part II: Terms and Conditions of NIH Grant Awards, Subpart A: General and Part II: Terms and Conditions of NIH Grant Awards, Subpart B: Terms and Conditions for Specific Types of Grants, Recipients, and Activities, including of note, but not limited to:
- Federalwide Research Terms and Conditions
- Prohibition on Certain Telecommunications and Video Surveillance Services or Equipment
- Acknowledgment of Federal Funding
If a recipient is successful and receives a Notice of Award, in accepting the award, the recipient agrees that any activities under the award are subject to all provisions currently in effect or implemented during the period of the award, other Department regulations and policies in effect at the time of the award, and applicable statutory provisions.
Should the applicant organization successfully compete for an award, recipients of federal financial assistance (FFA) from HHS must administer their programs in compliance with federal civil rights laws that prohibit discrimination on the basis of race, color, national origin, disability, age and, in some circumstances, religion, conscience, and sex (including gender identity, sexual orientation, and pregnancy). This includes ensuring programs are accessible to persons with limited English proficiency and persons with disabilities. The HHS Office for Civil Rights provides guidance on complying with civil rights laws enforced by HHS. Please see https://www.hhs.gov/civil-rights/for-providers/provider-obligations/index.html and https://www.hhs.gov/civil-rights/for-individuals/nondiscrimination/index.html
HHS recognizes that research projects are often limited in scope for many reasons that are nondiscriminatory, such as the principal investigator’s scientific interest, funding limitations, recruitment requirements, and other considerations. Thus, criteria in research protocols that target or exclude certain populations are warranted where nondiscriminatory justifications establish that such criteria are appropriate with respect to the health or safety of the subjects, the scientific study design, or the purpose of the research. For additional guidance regarding how the provisions apply to NIH grant programs, please contact the Scientific/Research Contact that is identified in Section VII under Agency Contacts of this FOA.
- Recipients of FFA must ensure that their programs are accessible to persons with limited English proficiency. For guidance on meeting the legal obligation to take reasonable steps to ensure meaningful access to programs or activities by limited English proficient individuals see https://www.hhs.gov/civil-rights/for-individuals/special-topics/limited-english-proficiency/fact-sheet-guidance/index.html and https://www.lep.gov.
- For information on an institution’s specific legal obligations for serving qualified individuals with disabilities, including reasonable accommodations and making services accessible to them, see http://www.hhs.gov/ocr/civilrights/understanding/disability/index.html.
- HHS funded health and education programs must be administered in an environment free of sexual harassment, see https://www.hhs.gov/civil-rights/for-individuals/sex-discrimination/index.html. For information about NIH's commitment to supporting a safe and respectful work environment, who to contact with questions or concerns, and what NIH's expectations are for institutions and the individuals supported on NIH-funded awards, please see https://grants.nih.gov/grants/policy/harassment.htm.
- For guidance on administering programs in compliance with applicable federal conscience protection and associated anti-discrimination laws see https://www.hhs.gov/conscience/conscience-protections/index.html and https://www.hhs.gov/conscience/religious-freedom/index.html.
Please contact the HHS Office for Civil Rights for more information about obligations and prohibitions under federal civil rights laws at https://www.hhs.gov/ocr/about-us/contact-us/index.html or call 1-800-368-1019 or TDD 1-800-537-7697.
In accordance with the statutory provisions contained in Section 872 of the Duncan Hunter National Defense Authorization Act of Fiscal Year 2009 (Public Law 110-417), NIH awards will be subject to the Federal Awardee Performance and Integrity Information System (FAPIIS) requirements. FAPIIS requires Federal award making officials to review and consider information about an applicant in the designated integrity and performance system (currently FAPIIS) prior to making an award. An applicant, at its option, may review information in the designated integrity and performance systems accessible through FAPIIS and comment on any information about itself that a Federal agency previously entered and is currently in FAPIIS. The Federal awarding agency will consider any comments by the applicant, in addition to other information in FAPIIS, in making a judgement about the applicant’s integrity, business ethics, and record of performance under Federal awards when completing the review of risk posed by applicants as described in 45 CFR Part 75.205 and 2 CFR Part 200.206 Federal awarding agency review of risk posed by applicants. This provision will apply to all NIH grants and cooperative agreements except fellowships.
Not Applicable
3. Reporting
When multiple years are involved, recipients will be required to submit the Research Performance Progress Report (RPPR) annually and financial statements as required in the NIH Grants Policy Statement.
A final RPPR, invention statement, and the expenditure data portion of the Federal Financial Report are required for closeout of an award, as described in the NIH Grants Policy Statement. NIH FOAs outline intended research goals and objectives. Post award, NIH will review and measure performance based on the details and outcomes that are shared within the RPPR, as described at 45 CFR Part 75.301 and 2 CFR Part 200.301.
The Federal Funding Accountability and Transparency Act of 2006 (Transparency Act), includes a requirement for recipients of Federal grants to report information about first-tier subawards and executive compensation under Federal assistance awards issued in FY2011 or later. All recipients of applicable NIH grants and cooperative agreements are required to report to the Federal Subaward Reporting System (FSRS) available at www.fsrs.gov on all subawards over $25,000. See the NIH Grants Policy Statement for additional information on this reporting requirement.
In accordance with the regulatory requirements provided at 45 CFR 75.113 and Appendix XII to 45 CFR Part 75, recipients that have currently active Federal grants, cooperative agreements, and procurement contracts from all Federal awarding agencies with a cumulative total value greater than $10,000,000 for any period of time during the period of performance of a Federal award, must report and maintain the currency of information reported in the System for Award Management (SAM) about civil, criminal, and administrative proceedings in connection with the award or performance of a Federal award that reached final disposition within the most recent five-year period. The recipient must also make semiannual disclosures regarding such proceedings. Proceedings information will be made publicly available in the designated integrity and performance system (currently FAPIIS). This is a statutory requirement under section 872 of Public Law 110-417, as amended (41 U.S.C. 2313). As required by section 3010 of Public Law 111-212, all information posted in the designated integrity and performance system on or after April 15, 2011, except past performance reviews required for Federal procurement contracts, will be publicly available. Full reporting requirements and procedures are found in Appendix XII to 45 CFR Part 75 Award Term and Conditions for Recipient Integrity and Performance Matters.
We encourage inquiries concerning this funding opportunity and welcome the opportunity to answer questions from potential applicants.
eRA Service Desk (Questions regarding ASSIST, eRA Commons, application errors and warnings, documenting system problems that threaten submission by the due date, and post-submission issues)
Finding Help Online: http://grants.nih.gov/support/ (preferred method of contact)
Telephone: 301-402-7469 or 866-504-9552 (Toll Free)
General Grants Information (Questions regarding application instructions, application processes, and NIH grant resources)
Email: [email protected] (preferred method of contact)
Telephone: 301-945-7573
Grants.gov Customer Support (Questions regarding Grants.gov registration and Workspace)
Contact Center Telephone: 800-518-4726
Email: [email protected]
Tamara Haegerich, Ph.D.
National Institute on Drug Abuse (NIDA)
Phone: 301-443-1185
Email: [email protected] (preferred method of contact)
Janet Kuramoto-Crawford, Ph.D.
National Institute on Drug Abuse (NIDA)
Phone: 301-443-8856
Email: [email protected] (preferred method of contact)
Wendy Weber, N.D., Ph.D., M.P.H.
National Center for Complementary and Integrative Health (NCCIH)
Telephone: 301-402-1272
Email: [email protected]
Laura Elizabeth Kwako, Ph.D.
National Institute on Alcohol Abuse and Alcoholism (NIAAA)
Phone: 301-451-8507
E-mail: [email protected]
Dharmendar Rathore, Ph.D.
National Institute on Drug Abuse (NIDA)
Phone: 301-402-6965
Email: [email protected]
Lennin GreenwoodNational Institute on Drug AbusePhone: 301-827-0478Email: [email protected]
Debbie Chen
National Center for Complementary and Integrative Health (NCCIH)
Phone: 301-594-3788
Email: [email protected]
Judy Fox
National Institute on Alcohol Abuse and Alcoholism (NIAAA)
Phone: (301) 443-4704
E-mail: [email protected]
Recently issued trans-NIH policy notices may affect your application submission. A full list of policy notices published by NIH is provided in the NIH Guide for Grants and Contracts. All awards are subject to the terms and conditions, cost principles, and other considerations described in the NIH Grants Policy Statement.
Awards are made under the authorization of Sections 301 and 405 of the Public Health Service Act as amended (42 USC 241 and 284) and under Federal Regulations 42 CFR Part 52 and 45 CFR Part 75.
and Human Services (HHS)